Patient Care Report (PCR) Documentation Guidelines s - GCHD
6 hours ago An essential part of the pre-hospital medical care is the documentation of the care provided, the medical condition, and history of the patient. The purpose of record documentation is to provide an accurate, comprehensive permanent record of each patient’s condition and the treatment rendered, as well as serving as a data collection tool. >> Go To The Portal
How to Write a Patient Care Report?
- Be More Specific Than Just Being General One thing you may take notice of or the first thing that you may take notice...
- Fill Out the Correct Details If your report is mostly like that of a checklist or a fill in the blanks type, remember...
- Write the Report Once the Call Is Made After you get the call it is always best to...
There are seven elements (at a minimum) that we have identified as essential components to documenting a well written and complete narrative.
- Dispatch & Response Summary. ...
- Scene Summary. ...
- HPI/Physical Exam. ...
- Interventions. ...
- Status Change. ...
- Safety Summary. ...
- Disposition.
How do you write a patient care report?
- Recognition and description of a new disease
- Recognition of rare manifestations of a known disease
- Elucidation of the mechanisms of a disease
- Detection of adverse or beneficial side effects of drugs (and other treatments)
- Medical education and audit
How to write a patient care report?
Patient-Centered Care Report example
- Attach a reference list to your report. ...
- Describe the outcomes that were not achieved, the extent to which they fell short of expectations, and any variance across demographic groups.
- Identify the factors (for example: institutional, community, environmental, resources, communication) that may have contributed to any achievement shortfalls. ...
How to write a better EMT patient care report?
- Each PCR should include all pertinent times associated with the EMS call.
- As well as the times of the assessments and treatments provided, the PCR should include detailed signs and symptoms and other assessment findings such as vital signs, and all the ...
- Also documented are changes in patient condition after treatment.
How to create a patient medical summary report?
Writing a good medical report
- The Medico-Legal Report in Emergency Medicine. Emergency Medicine 1995:7;233.
- Abstract. The preparation of a medico-legal report is an exercise in communication between the doctors and the legal system.
- Introduction. ...
- The request. ...
- Consent. ...
- Format. ...
- A suggested structure is: Data such as the time, date and place, and the reason for the examination. ...
- Conclusion. ...
What should be included in a patient care report?
What Patient Care Reports Should IncludePresenting medical condition and narrative.Past medical history.Current medications.Clinical signs and mechanism of injury.Presumptive diagnosis and treatments administered.Patient demographics.Dates and time stamps.Signatures of EMS personnel and patient.More items...•
How do you write a patient report?
Summary: The format of a patient case report encompasses the following five sections: an abstract, an introduction and objective that contain a literature review, a description of the case report, a discussion that includes a detailed explanation of the literature review, a summary of the case, and a conclusion.
How do you write a good PCR?
How to Write an Effective ePCR NarrativeBe concise but detailed. Be descriptive in explaining exactly what happened and include the decision-making process that led to the action. ... Present the facts in clear, objective language. ... Eliminate incorrect grammar and other avoidable mistakes. ... Be consistent and thorough.
What the patient care report represents?
More Definitions of Patient care report Patient care report means the written documentation that is the official medical record that documents events and the assessment and care of a patient treated by EMS professionals.
How do you start a report?
The first section you start writing in your report is always a summary or introduction. This should stretch across just one or two pages to give your reader a brief glimpse into what your results or findings are.
How do you write a nursing patient report?
How to write a nursing progress noteGather subjective evidence. After you record the date, time and both you and your patient's name, begin your nursing progress note by requesting information from the patient. ... Record objective information. ... Record your assessment. ... Detail a care plan. ... Include your interventions.
How do you write a patient assessment?
Assessment & PlanWrite an effective problem statement.Write out a detailed list of problems. From history, physical exam, vitals, labs, radiology, any studies or procedures done, microbiology write out a list of problems or impressions.Combine problems.
What is a PCR report?
PCR means polymerase chain reaction. It's a test to detect genetic material from a specific organism, such as a virus. The test detects the presence of a virus if you have the virus at the time of the test. The test could also detect fragments of the virus even after you are no longer infected.
What is a PCR in writing?
The PARCC Summative Assessments in Grades 3-11 will measure writing using three prose constructed response (PCR) items. In the classroom writing can take many forms, including both informal and formal.
What is EMS document?
Documents are an important element of an environmental management system (EMS) as they provide written evidence of procedures, records and instructions. They can also provide a history of the EMS, enabling you to check whether improvements are continuing to being made.
What is the minimum data set in a patient care report?
The Minimum Data Set (MDS) is part of a federally mandated process for clinical assessment of all residents in Medicare or Medicaid certified nursing homes. This process entails a comprehensive, standardized assessment of each resident's functional capabilities and health needs.
How do you write EMS?
0:4011:38How to Write a Narrative in EMS || DCHART Made Easy ... - YouTubeYouTubeStart of suggested clipEnd of suggested clipName in parentheses. Now we know who all was on this call paramedic jackson advanced emt smith andMoreName in parentheses. Now we know who all was on this call paramedic jackson advanced emt smith and nremt. White then i talk about what happened while i was in route to the call.
What is the format for report writing?
Report writing is a formal style of writing elaborately on a topic. The tone of a report and report writing format is always formal. The important section to focus on is the target audience. For example – report writing about a school event, report writing about a business case, etc.
How do you write a diagnosis report?
Guidelines for Writing Diagnostic ReportsThe Appearance of the Diagnostic Report. ... The "Shelf Life" of the Disability Documentation. ... The Reason for Referral and History of the Problem. ... Evaluation Measures Used in the Report. ... Relevant Developmental, Educational and Medical Histories. ... A Clear Statement of the Disability.More items...
How do you prepare a case report?
Ten Steps to Writing an Effective Case Report (Part 1)Step 1: Identify the Category of Your Case Report. ... Step 2: Select an Appropriate Journal. ... Step 3: Structure Your Case Report According to the Journal Format. ... Step 4: Start Writing. ... Step 5: Collect Information Related to the Case.
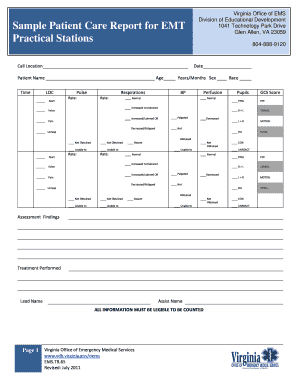
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the inf...
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very caref...
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make...
What to Include on a Patient Care Report (ePCR)
Accurate patient data is arguably the most valuable tool a medic has at his or her disposal. It not only informs immediate treatment decisions, but it shows what is – and isn’t – working. It plays a pivotal role in efficient patient hand-off at the ED, and it dictates the type of care he or she will receive in the minutes and hours after.
ePCRs: Patient Care Reports for the 21 st Century
Over the last 30 years, EMS agencies and hospitals alike have recognized the value of going digital with patient records, coining the term “electronic patient care reports” (ePCRs).
About Patient Care Reports
Digital patient care reports are slowly but surely changing the way patient information is recorded on a call, but they do not change interactions with patients. Instead of jotting down notes on a paper form, medics quickly and easily record the same information using a tablet and a digital form.
What Patient Care Reports Should Include
Just like the paper version of patient care reports, ePCRs are meant to be complete and contain all pertinent information to help deliver proper patient treatment and track performance metrics.
Obstacles to Efficiently Creating Electronic Patient Care Reports
As the adoption of ePCRs has ramped up in the last three decades, technology has evolved along with it. However, technology includes its own set of challenges. Onboarding an entire EMS agency to a new records system takes a coordinated effort and can require a substantial investment in time and money.
Comparing Documentation Methods: SOAP vs. CHART vs. IMRaD
Accurate, complete, and rich documentation in patient care reports can improve patient outcomes, provide accurate claims processing, further quality assurance, and even defend against malpractice. Offering guidance on what elements to include in narratives can result in more complete run reports.
New ePCRs Improve Patient Care While Improving Analytics and Reporting
Today’s top ePCR software tools offer direct improvement to patient care by streamlining communication and reducing the chance for human error. For example, customized forms in the system can be progressive, meaning a medic cannot move on to the next field without recording data for all required fields first.
What Do Patient Reports Look Like?
In order to write patient case reports, the content is divided into five elements: the abstract, an introduction that will contain a written review, a description of that review, a discussion entitled “Why does the literature review matter?”, a summary about how it may relate and finally conclusion.”.
What Is Pcr In Medical Billing?
An PCR document serves as a summary of an individual’s permanent medical record as well as one that documents the event they’re having. It constitutes the basis for medical billing claims.
Why Is It Important To Write A Good Patient Care Report?
It’s crucial to accurately reflect this level of patient care, regardless of how well it’s delivered. Likewise, in receiving facilities, good written guidelines may serve as guides for what treatment or treatment plans are to follow for patients previously received.
What Is The Purpose Of Patient Care?
Health outcomes can very well be affected if quality patient care is given. People suffering from illnesses such as cancer are more likely to experience higher levels of depression and improved health outcomes when offered this service.
How Do You Write A Good Patient Care Report Part 2?
Make sure the terms you use are clear. Use neutral words and phrases like “weakness” and “fall” or “transport for high-level care in your nursing communication. These terms don’t provide an accurate picture of the signs and symptoms in the patient at the time of transportation, so aim to be as specific as possible.
What Should Be Included In A Patient Report?
It is proposed that the document include elements of background information, medical records, physical examinations, specimens obtained, treatment options and opinions.
Watch what is a patient care report Video
What Intervention Demonstrates The Integration Of Patient Centered Care?
Health Care Report Template Details
The following are some specifics of patient care report form. Prior to fill in the form, it is usually definitely worth reading m ore details on it. Learn more... Hide more
Over 1 Million Users Love FormsPal
We are happy to have been very useful for a huge number of citizens with their different PDF documents by offering our easy-to-follow and accessible PDF editor.There exists a means by which we may help you as well, since you're here!
What to ask for in a case report?
It is often best to ask for informed consent and the patient’s perspective before you begin writing your case report. Appendices (If indicated). Submission to a scientific journal. Follow author guidelines and journal submission requirements when writing and submitting your case report to a scientific journal.
Do you need informed consent for a journal?
The patient should provide informed consent (including a patient perspective) and the author should provide this information if requested. Some journals have consent forms which must be used regardless of informed consents you have obtained. Rarely, additional approval (e.g., IRB or ethics commission) may be needed.
Why are patient reports important?
Why Patient Reports Are Needed. Patient medical reports serve as evidences that the patient has been given proper medications or treatments. Doctors or physicians are doing the best they could in order to supply the needs of each and every patient, regardless if they are in a critical condition or not.
What is the relevant information needed for a patient complaint?
In a patient complaint, the relevant information that are needed are as follows: The description of the situation. The effect on privacy.
What is healthcare personnel?
Healthcare personnel in hospitals or medical centers ensure that they provide the needs of the patients (pertaining to the treatments or medications needed) and their individual relatives (pertaining to the answers or provision of exact details from the medical results). It goes without saying that everyone wants an accurate general information ...
Do hospitals keep records of patients?
Therefore, it is mandatory that the medical clinic, center, or hospital keeps a record of their patients. These patient reports also help the doctors and the relatives of the patient to know what is or are behind the patients’ results of their individual health assessment.
Can results from medical assessments be given due to deficiency of relevant information?
Otherwise, results from medical assessments cannot be given due to deficiency of relevant information.