The nurse is gathering data on a patient which data
35 hours ago Inspecting the condition of a surgical incision or wound, describing an observed behavior, and measuring blood pressure are examples of objective data. States “doesn’t feel good,” reports a headache, and nausea are all subjective data. Subjective data include the patient’s feelings, perceptions, and reported symptoms. >> Go To The Portal
Objective data is factual information that professionals gather through observation or measurement that is true regardless of the feelings or opinions of the person presenting or receiving the information. Examples of objective data in nursing include blood pressure and heart rate.
The nurse is gathering data on a patient. Which data will the nurse report as objective data? Rationale: Objective data are observations or measurements of a patient's health status, like respirations.
Full
AnswerWhen does the nurse need to analyze the data collected?
After assessment and documentation of the information obtained from the client, the nurse needs to analyze the data collected. Which nursing actions depend on accurate analysis of data during this phase of the nursing process? Select all that apply.
What is objective data in nursing?
Objective data in nursing refers to information that can be measured through physical examination, observation, or diagnostic testing. Examples of objective data include, but are not limited to, physical findings or patient behaviors observed by the nurse, laboratory test results, and vital signs.
What does the nurse discover after reviewing the database?
After reviewing the database, the nurse discovers that the patient's vital signs have not been recorded by the nursing assistive personnel (NAP). Which clinical decision should the nurse make?
What does the nurse use results from diagnostic and laboratory tests for?
The nurse uses results from the diagnostic and laboratory tests to establish a patient database, not checking orders for tests. A nurse is gathering information about a patient's habits and lifestyle patterns. Which method of data collection will the nurse use that will best obtain this information?
Which data collected during the nurse patient interview is a subjective finding?
Subjective data include the patient's feelings, perceptions, and reported symptoms.
Which is considered objective data obtained from the patient?
Objective data is information obtained using our senses. If you can see, smell, touch, taste, or feel it, then it's either measured or observed and is an example of objective data.
Which client information would the nurse report as subjective data?
Symptoms, values, perceptions, feelings, beliefs, attitudes, and sensations are sources of subjective data. A nurse performing triage in an emergency room makes assessments of clients using critical thinking skills.
Which part of the nursing process gathers information about the patient?
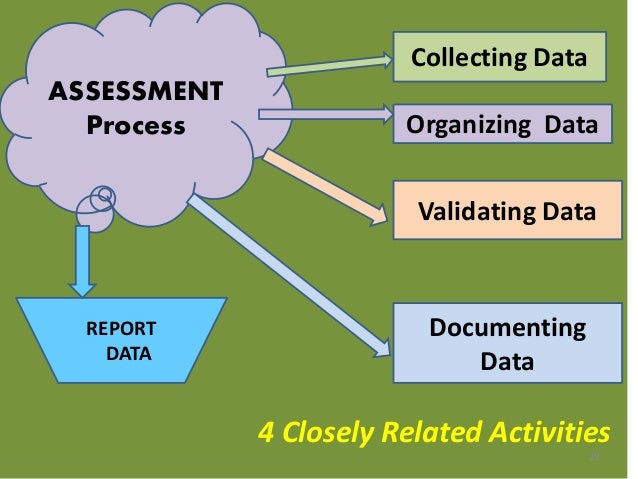
the assessment phaseThe first phase of the nursing process is the assessment phase. In this phase, the nurse collects and organizes data related to the patient. Data includes information about the patient, family, caregivers, or the patient's community or environment as it is relevant to his health and well-being.
What is objective data in nursing?
Objective data in nursing refers to information that can be measured through physical examination, observation, or diagnostic testing. Examples of objective data include, but are not limited to, physical findings or patient behaviors observed by the nurse, laboratory test results, and vital signs.
What is an example of objective data?
Examples of objective data are vital signs, physical examination findings, and laboratory results. An example of objective data is recording a blood pressure reading of 140/86. Subjective data and objective data are often recorded together during an assessment.
What is objective information in the medical field?
Objective evidence refers to visible, measurable findings obtained by a medical examination, tests, or diagnostic imaging. Someone other than the injured worker must be able to see or feel the evidence. Examples of objective evidence include a broken leg or an abrasion.
What are subjective data examples?
Subjective data is going to be information that you receive from the patient or from one of his or her knowledgeable companions....Here are some Examples of Subjective Data Findings:Pain.Shortness of breath.Dizziness.Exhaustion.Itching.Coughing.Vomiting.
Is Vital Signs objective or subjective?
objectiveVital signs are an objective measurement of the essential physiological functions of a living organism. They have the name "vital" as their measurement and assessment is the critical first step for any clinical evaluation.
What is objective and subjective data in nursing?
Subjective nursing data is information that depends on personal feelings, while objective nursing data is factual information. Nurses can collect objective and subjective data from patients, family members, other doctors and medical technicians to develop a holistic understanding of a patient's health.
How do you find objective data?
How to Get Objective Data. Objective data is obtained as soon as the nurse sees the patient. This involves reading the patient's body language and noticing specific behaviors. The type of eye contact, body positions and hand gestures a patient makes can be the first information that is collected.
What sources does the nurse use to gather data?
The primary methods used to collect data are observing, interviewing, and examining. Observation occurs whenever the nurse is in contact with the client or support persons. Interviewing is used mainly while taking the nursing health history. Examining is the major method used in the physical health assessments.
What does a nurse speak to?
B. The nurse speaks only to the patient's daughter. Gathering data from family members is acceptable, but when a patient is able to interact, nurses need to include information from the older adult to complete the assessment. Therefore, the charge nurse must correct this misconception.
What is the difference between data interpretation and validation?
Validation, by definition, involves comparing data with other sources for accuracy. Data interpretation involves identifying abnormal findings, clarifying information, and identifying patient problems. The nurse should validate data before interpreting the data and making inferences.
What is a nursing database?
A nursing database includes a physical examination. The nurse reviews the current literature in the implementation phase of the nursing process to determine evidence-based actions, and the health care provider is responsible for ordering medications.
What should a nurse do after setting the agenda?
After setting the agenda, the nurse should conduct the actual interview and proceed with data collection, such as asking about the patient's current chief concerns or problems. Introductions occur before setting the agenda.
What validates a patient's report with a nurse's observation?
The only scenario that validates a patient's report with a nurse's observation is changing the wound dressing. The nurse validates what the patient says by observing the dressing. The rest of the examples have the nurse acting only from a patient and/or family reports, not the nurse's assessment.
Should a nurse record vital signs?
The nurse should ask the nursing assistive personnel to record the vital signs for review before administering medicines or transporting the patient to another department. The nurse should not make assumptions when providing high-quality patient care, and omitting the vital signs is not an appropriate action.
When assessing an older adult, do nurses need to listen carefully and allow the patient to speak?
When assessing an older adult, nurses need to listen carefully and allow the patient to speak. Positive nonverbal communication, such as making eye contact, nodding, and lean ing forward, shows interest in the patient. Thus, the charge nurse does not need to intervene or follow up. A nurse is completing an assessment.
What should a nurse do before a physical exam?
Before the physical examination, the nurse should first. A. take a complete health history. B. collect all home medications brought to the hospital.
What is clinical instructor?
A clinical instructor is teaching a nursing student group about organizing data when documenting and communicating assessment findings. The clinical instructor knows that the method being taught promotes critical thinking and clustering of similar data.
What does a nurse emphasize when answering questions about health during a presentation at a women's club lunche
When answering questions about health during a presentation at a women's club luncheon, the nurse emphasizes that prevention of disease is multifaceted but is connected directly to. A. a healthy lifestyle.
Do nurses need to think critically?
C. Nurses do not need to think critically; they just need to follow the doctor's orders. D. Critical thinking helps nurses decide which parts of the nursing process are not needed in regard to a particular client. C. Complete health history. A nurse performs a comprehensive assessment on a client.

Popular Posts:
- 1. www./patient services@"imp wellness center."com/patient-login follow my health
- 2. family practice center patient portal
- 3. patient portal diagnostic clinic moberly mo
- 4. women's health services patient portal
- 5. largest homehealth care ohio patient portal
- 6. pmg the heights patient portal
- 7. st joseph patient portal sy rny
- 8. az mmj patient portal
- 9. lamia kadir md patient portal
- 10. e; rio patient portal