Patient Progress Report Template - PDF Templates
2 hours ago E), and the Progress Report Section (Part F). Continuing a QIS with Modifications. 3 . Complete the Background Information Section (Parts B and C); Implementation Plan Section (Parts D and E); and the Progress Report Section (Part F). 1 . A “new QIS” is defined as a QIS that has not been previously submitted to a Marketplace, or is a QIS ... >> Go To The Portal
What is the purpose of a Medicare progress report?
Terminate services, if necessary (see the discharge note section below). According to Jewell and Wallace, “The Medicare progress report is intended to address the patient’s progress toward his or her goals as noted in the established plan of care.
What is the proper format for a progress note for Medicare?
There is no particular format required by Medicare as long as all the above is contained in the note as long as it happens at least once every 10 treatment visits. When co-treating a patient with a PTA or OTA the PT or OT must personally provide one full billable service on one date of service (DOS) within that progress note period.
What is included in a patient progress report template?
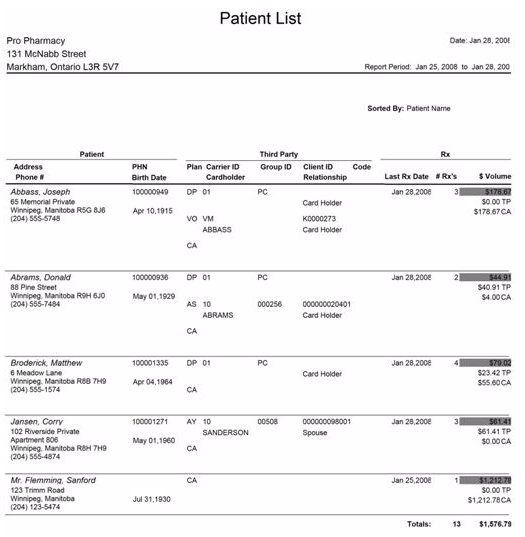
This Sample Patient Progress Report Template has the patient's personal information, physiological and psychological health progress. The progress report specifies the patient's mood, communication, appearance, emotional status, mental stability, interventions, and respond to treatment, and the report summary.
What is a patient report form?
Report Forms FREE 14+ Patient Report Forms in PDF | MS Word Healthcare personnel in hospitals or medical centers ensure that they provide the needs of the patients (pertaining to the treatments or medications needed) and their individual relatives (pertaining to the answers or provision of exact details from the medical results).
What is the purpose of Part B documentation?
From Medicare’s perspective, the primary purpose of all Part B documentation is to demonstrate that the care fully supports the medical necessity of the services provided. That means a Progress Report must clearly describe how the services are medically necessary for that patient.
Can progress reports be billed separately?
It’s also important to remember the time involved in writing a progress report cannot be billed separately. Like all documentation, Medicare considers it included in the payment for the treatment time charge. Progress Reports do not need to be a separate document from a daily treatment note.
What is a plan of care for Medicare?
When treating Medicare patients, the Plan of Care refers to the written treatment plan for which the intended therapy services must specifically relate to. The Plan of Care is established at the time of the first visit with the patient and is derived from the clinical information gathered during the Initial Therapy Evaluation.
Can Medicare deny POCs?
Since Medicare could potentially deny or claw back payment if the above time frames are not met, it is essential that your practice establish a workflow to keep track of Medicare POCs and Progress Reports. If your EMR does not offer a tracking system, then this may end up being a manual process using home grown spreadsheets or some other recording method. However, if you are an OptimisPT user, you can take advantage of the embedded alerts, reminders and reports that can track this for you.
Background Information
All citations are detailed in References list at the end of this topic.
Establishing a Plan of Care
In documentation for Medicare patients, an alert appears when reviewing the Case information to indicate that the Plan of Care has not yet been established:
Entering Plan of Care Information
Follow these steps to enter Plan of Care information for the patient in the Client Editor:
Handling Plan of Care Expiration
Follow these steps to update Plan of Care information when the current Plan of Care expires:
Why are patient reports important?
Why Patient Reports Are Needed. Patient medical reports serve as evidences that the patient has been given proper medications or treatments. Doctors or physicians are doing the best they could in order to supply the needs of each and every patient, regardless if they are in a critical condition or not.
What is the relevant information needed for a patient complaint?
In a patient complaint, the relevant information that are needed are as follows: The description of the situation. The effect on privacy.
What is healthcare personnel?
Healthcare personnel in hospitals or medical centers ensure that they provide the needs of the patients (pertaining to the treatments or medications needed) and their individual relatives (pertaining to the answers or provision of exact details from the medical results). It goes without saying that everyone wants an accurate general information ...
Do hospitals keep records of patients?
Therefore, it is mandatory that the medical clinic, center, or hospital keeps a record of their patients. These patient reports also help the doctors and the relatives of the patient to know what is or are behind the patients’ results of their individual health assessment.
Can results from medical assessments be given due to deficiency of relevant information?
Otherwise, results from medical assessments cannot be given due to deficiency of relevant information.
How often do you need a progress note for Medicare?
Currently, Medicare only requires a progress note be completed, at minimum, on every 10th visit. I hope that helps!
What is a progress note for a therapist?
In it, the therapist must: Include an evaluation of the patient’s progress toward current goals. Make a professional judgment about continued care.
How long does it take for Medicare to recertify?
And even when things do go according to plan, Medicare requires recertification after 90 days of treatment. If you’re a WebPT Member, you can use WebPT’s Plan of Care Report to identify which plans of care are still pending certification as well as which ones require certification—before those 90 days are up.
What is a POC in therapy?
The Plan of Care (POC) Based on the assessment, the therapist then must create a POC —complete with treatment details, the estimated treatment time frame, and the anticipated results of treatment. At minimum, Medicare requires the POC to include: Medical diagnosis. Long-term functional goals.
How long does it take to sign a POC?
Medicare requires that a licensed physician or nonphysician practitioner (NPP) date and sign the POC within 30 days. To make things easier, though, the certifying physician doesn’t have to be the patient’s regular physician—or even see the patient at all (although some physicians do require a visit).
How long does it take for Medicare to discharge a patient?
Medicare automatically discharges patients 60 days after the last visit. Unfortunately, if the patient has been discharged, then you will need to perform a new initial evaluation. If you do not live in a direct access state, then you will also need to to get the physician's signature on the patient's new POC.
What is the evaluation of a licensed therapist?
Before starting treatment, the licensed therapist must complete an initial evaluation of the patient, which includes: Objective observation (e.g., identified impairments and their severity or complexity) And, of course, all of this should be accounted for you in your documentation.
Your Chiropractic Assessment and Evaluation
Use this Updated Chiropractic Patient History to record changes in their symptoms and produce a written assessment of the progress of their chiropractic care.
Your Re-evaluation Proves Medical Necessity
Is your treatment plan working? Insurance companies expect that you’ll prove your value with periodic updates and assessments. Taking a proper history, especially at the re-evaluation, gives you a position of strength as you proactively justify the need for continued chiropractic care.
What is Medicare Administrative Contractor?
The Medicare Administrative Contractor is hereby advised that this constitutes technical direction as defined in your contract. CMS does not construe this as a change to the MAC Statement of Work. The contractor is not obligated to incur costs in excess of the amounts allotted in your contract unless and until specifically authorized by the Contracting Officer. If the contractor considers anything provided, as described above, to be outside the current scope of work, the contractor shall withhold performance on the part(s) in question and immediately notify the Contracting Officer, in writing or by e-mail, and request formal directions regarding continued performance requirements.
What is an initial evaluation?
The initial evaluation, or the plan of care including an evaluation, should document the necessity for a course of therapy through objective findings and subjective patient self-reporting. Utilize the guidelines of the American Physical Therapy Association, the American Occupational Therapy Association, or the American Speech-Language and Hearing Association as guidelines, and not as policy. Only a clinician may perform an initial examination, evaluation, re-evaluation and assessment or establish a diagnosis or a plan of care. A clinician may include, as part of the evaluation or re-evaluation, objective measurements or observations made by a PTA or OTA within their scope of practice, but the clinician must actively and personally participate in the evaluation or re-evaluation. The clinician may not merely summarize the objective findings of others or make judgments drawn from the measurements and/or observations of others.
What is physical therapy?
Physical therapy services are those services provided within the scope of practice of physical therapists and necessary for the diagnosis and treatment of impairments, functional limitations, disabilities or changes in physical function and health status. (See Pub. 100-03, the Medicare National Coverage Determinations Manual, for specific conditions or services.) For descriptions of aquatic therapy in a community center pool see section 220C of this chapter.
What is the purpose of a treatment note?
The purpose of these notes is simply to create a record of all treatments and skilled interventions that are provided and to record the time of the services in order to justify the use of billing codes on the claim. Documentation is required for every treatment day, and every therapy service. The format shall not be dictated by contractors and may vary depending on the practice of the responsible clinician and/or the clinical setting.
Is speech language pathology a Medicare insured?
Services of speech-language pathology assistants are not recognized for Medicare coverage. Services provided by speech-language pathology assistants, even if they are licensed to provide services in their states, will be considered unskilled services and denied as not reasonable and necessary if they are billed as therapy services.
Can an occupational therapy assistant write a progress report?
Occupational Therapy Assistants may write elements of the Progress Report dated between clinician reports. Reports written by assistants are not complete Progress Reports. The clinician must write a Progress Report during each Progress Report Period regardless of whether the assistant writes other reports. However, reports written by assistants are part of the record and need not be copied into the clinicians report. Progress Reports written by assistants supplement the reports of clinicians and shall include:
Can a therapist bill Medicare?
In order to qualify to bill Medicare directly as a therapist, each individual must be enrolled as a private practitioner and employed in one of the following practice types: an unincorporated solo practice, unincorporated partnership, unincorporated group practice, physician/NPP group or groups that are not professional corporations, if allowed by state and local law. Physician/NPP group practices may employ physical therapists in private practice (PTPP) and/or occupational therapists in private practice (OTPP) if state and local law permits this employee relationship.
When to Use A Progress Report vs. A Plan of Care When Treating Medicare Patients
By:Jennifer Heiligman, PT, MPT We all know Medicare likes to keep us on our toes in terms of outpatient rehab therapy documentation requirements. In addition, those requirements are not always communicated in the clearest manner possible. Take for instance, the question “Do I need a Progress Report or a Plan of Care?” B…
Plan of Care
- When treating Medicare patients, the Plan of Care refers to the written treatment plan for which the intended therapy services must specifically relate to. The Plan of Care is established at the time of the first visit with the patient and is derived from the clinical information gathered during the Initial Therapy Evaluation. Per Medicare, the minimal information required in the Plan of Car…
Progress Reports
- A Progress Report provides justification for the medical necessity of the skilled therapy being provided to the patient. Per Medicare, a Progress Report should include: 1. Objective evidence to support the need for skilled treatment 1.1. This includes such things as validated functional outcome measures and standardized patient assessment tools. Th...
Staying Compliant with Time Frames
- Since Medicare could potentially deny or claw back payment if the above time frames are not met, it is essential that your practice establish a workflow to keep track of Medicare POCs and Progress Reports. If your EMR does not offer a tracking system, then this may end up being a manual process using home grown spreadsheets or some other recording method. However, if y…
Establishing A Plan of Care
- In documentation for Medicare patients, an alert appears when reviewing the Case information to indicate that the Plan of Care has not yet been established: After the Plan of Care has been established in the initial evaluation, double click on the Case Name to open the Client Editor and enter the duration of the Plan of Care:
Entering Plan of Care Information
- Follow these steps to enter Plan of Care information for the patient in the Client Editor: 1. In the Client Editor, click the Add POC button. 1. The effective date will default to the date that the evaluation is being performed, but may be adjusted if necessary. The duration of the POC will normally default to 90 days: But you can adjust the duration date for Plans of Care less than 90 …
Handling Plan of Care Expiration
- Follow these steps to update Plan of Care information when the current Plan of Care expires: 1. The Case Information will alert the therapist when the current Plan of Care expires and when a new Progress Report is required. 2. To update the system after a Progress Report has been completed, click on Edit Plan of Care Dates, then the Add Prog Report...
References
- The one notable exception is CORFs. There is some specific language stating that in CORFs the Plan of Care can only be established by a physician. Respiratory Therapists working in CORFs only have...
- Medicare Benefits Policy Manual, Section 220.1.2 https://www.cms.hhs.gov/manuals/downloads/bp102c15.pdf
- The one notable exception is CORFs. There is some specific language stating that in CORFs the Plan of Care can only be established by a physician. Respiratory Therapists working in CORFs only have...
- Medicare Benefits Policy Manual, Section 220.1.2 https://www.cms.hhs.gov/manuals/downloads/bp102c15.pdf
- Medicare Benefits Policy Manual, Section 220.1.2, page 150https://www.cms.hhs.gov/manuals/downloads/bp102c15.pdf
- Federal Register, p. 185: https://a257.g.akamaitech.net/7/257/2422/01jan20071800/edocket.access.gpo.gov/2007/pd…
Popular Posts:
- 1. failure of paramedic to give handoff report to a nurse patient abandonment
- 2. nexus portal patient
- 3. how to get a login to tanner patient portal
- 4. lutheran general patient portal
- 5. patient portal st. joseph's hospital, syracuse ny
- 6. cfcardio patient portal
- 7. adam callahan's patient portal
- 8. st francis jennings patient portal
- 9. houston family practice patient portal
- 10. healthwise integrative medicine patient portal