FREE 14+ Patient Report Forms in PDF | MS Word
36 hours ago Step 3: Report the specimens. Whatever test and examination that you have given to the patient, have the result documented. These will be the laboratory results and test results to have an analysis of what disease could have touched the patient. There should be a clear notation how you have derived the specimens. >> Go To The Portal
What is included in a patient report?
Patient Report – Next on the report, is the Patient Report section. The Patient Report is tasked with collecting the medical details of the patient. These details include medical details such as the Diagnosis, Allergy Information, Medical History, and Code Status.
What are the benefits of patient report forms?
Therefore, one thing that could help are the patient report forms. These are used to summarize the overall findings from the diagnosis of a patient assessment, thus, making it easier to display and explain the results briefly yet comprehensively. Generic Patient Report Form
What is the file size of the patient report form?
File Format DOC Size: 581 KB Download Patient’s Adverse Event Report Form astrazeneca.com Details File Format PDF Size: 1 MB Download Request for Patient’s Medical Report Form ha.org.hk Details File Format PDF Size: 234 KB Download The Parts of Patient Report Forms
What are the benefits of nursing report sheets?
Due to their excellent recording system, nursing report sheets are used by physicians, doctors, nurses and other healthcare staff all over the world. These report sheets are highly beneficial in helping the medical staff to obtain information efficiently.
How do I create a nursing report sheet?
0:0020:45How to Give a Nursing Shift Report - YouTubeYouTubeStart of suggested clipEnd of suggested clipSo to get that you can go to our website registered nurse RN comm. Go to the search bar which is atMoreSo to get that you can go to our website registered nurse RN comm. Go to the search bar which is at the top right and type nursing report templates or nursing report sheets.
How do I fill out report sheet?
0:025:46FILLED IN REPORT SHEET - YouTubeYouTubeStart of suggested clipEnd of suggested clipAnd then I have their admitting diagnosis. When they are admitted in history and accidentallyMoreAnd then I have their admitting diagnosis. When they are admitted in history and accidentally flipped these around. So this was the admitting diagnosis. Across them or admitting.
How do you write a nursing patient report?
How to write a nursing progress noteGather subjective evidence. After you record the date, time and both you and your patient's name, begin your nursing progress note by requesting information from the patient. ... Record objective information. ... Record your assessment. ... Detail a care plan. ... Include your interventions.
What should a nursing report include?
What to cover in your nurse-to-nurse handoff reportThe patient's name and age.The patient's code status.Any isolation precautions.The patient's admitting diagnosis, including the most relevant parts of their history and other diagnoses.Important or abnormal findings for all body systems:More items...•
How do you write a simple report?
How to write a report in 7 steps1 Choose a topic based on the assignment. Before you start writing, you need to pick the topic of your report. ... 2 Conduct research. ... 3 Write a thesis statement. ... 4 Prepare an outline. ... 5 Write a rough draft. ... 6 Revise and edit your report. ... 7 Proofread and check for mistakes.
What makes a good report?
An effective report presents and analyses facts and evidence that are relevant to the specific problem or issue of the report brief. All sources used should be acknowledged and referenced throughout, in accordance with the preferred method of your department.
How do you write a patient report?
III. Patient case presentationDescribe the case in a narrative form.Provide patient demographics (age, sex, height, weight, race, occupation).Avoid patient identifiers (date of birth, initials).Describe the patient's complaint.List the patient's present illness.List the patient's medical history.More items...•
What is reporting in nursing practice?
Reporting is the verbal or written communication of data regarding the clients health status needs, treatments, outcomes and responses. Reporting facilitates clinical decision making, continuity of care and co-ordination among health team members.
How do you write patient notes?
9:1510:21How to Write Clinical Patient Notes: The Basics - YouTubeYouTubeStart of suggested clipEnd of suggested clipBut if you're on a paper record make sure you record that and finally make sure it's very clear whoMoreBut if you're on a paper record make sure you record that and finally make sure it's very clear who you are. So you print your name. You sign your name and then you have some sort of designation.
How do you do nursing documentation?
Tips for Great Nursing DocumentationBe Accurate. Write down information accurately in real-time. ... Avoid Late Entries. ... Prioritize Legibility. ... Use the Right Tools. ... Follow Policy on Abbreviations. ... Document Physician Consultations. ... Chart the Symptom and the Treatment. ... Avoid Opinions and Hearsay.More items...
What are the types of reports in nursing?
There are different types of nursing reports described in the literature, but the four main types are: a written report, a tape-recorded report, a verbal face-to-face report conducted in a private setting, and face-to-face bedside handoff.
What is SBAR template?
SBAR is an acronym for Situation, Background, Assessment, Recommendation. It is a technique used to facilitate appropriate and prompt communication. An SBAR template will provide you and other clinicians with an unambiguous and specific way to communicate vital information to other medical professionals.
Who Writes the Patient Medical Report?
Health care providers do the patient medical report. The health care professionals make the documentation for a patient. It includes all the physic...
Who Can Have Access to a Patient Medical Report?
The health care providers have the access to the patient medical report. They keep the medical report as a history of medical records. Also, patien...
Is a Patient Medical Report a Legal Document?
If it is signed by a health care professional, then it is a legal document. It is permissible in any court of law. It is an evidence that the patie...
Why is a mental health nursing report important?
It allows nurses and doctors to continue treating and providing care to their patients even when during shift interchange.
Why is it important to have an ICU nurse report?
Due to this, it is very important that nurses are able to gather the required information. To help with this situation, ICU Nursing Reports were brought into action. ICU Nursing Reports are used to obtain a list of essential details regarding the patient who has been admitted to the ICU.
What is a nursing report sheet?
The report sheets enable the nurses to record clear information regarding details including the diagnosis, history, allergies, consults, vital signs, lab results, and other such health-related data. Due to their excellent recording system, nursing report sheets are used by physicians, doctors, nurses and other healthcare staff all over the world. ...
Why do nurses use advance notes?
Advance notes to prompt nurses about the duties that they need to perform in the next shift. Moreover, nursing report sheets play a huge role in favor of the nurse’s life as well. Due to the vast expanse of the information present, a lot of nurses consider the reports to be akin to a secondary brain.
What is the purpose of the General Information section in a nursing report?
This section is responsible for generating all the details regarding the patient such as Date of Birth, Gender etc. of the patient.
What is flow sheet in nursing?
A6. In simple terms, a flow sheet is a single or dual-page form, tasked with the job of gathering all important aspects of a patient’s condition. Similar to the other nursing reports, the flow sheet is tasked with gathering patient information.
What is a lab report?
Labs – Labs refers to the various patient reports which have been derived from the numerous tests conducted on the patient. The constituents of this section are Labs, Needed Labs, and Future Procedures. Completion – Completion is the final section of a nursing report template.
What is a Patient Medical Report?
A patient medical report is a comprehensive document that contains the medical history and the details of a patient when they are in the hospital. It can also be given as a person consults a doctor or a health care provider. It is a proof of the treatment that a patient gets and of the condition that the patient has.
What You Should Include in a Patient Medical Report
A patient medical report has some important elements that you should not forget. Include all these things and you can learn how to write a patient medical report.
Importance of a Patient Medical Report
The reason why a patient medical report is always given is because it is important. Here, you can know some of the importance of a patient medical report:
How to Write a Good Patient Medical Report
A doctor is a doctor. They are not writers. They can be caught in a difficulty on how to write a patient medical report. If this is the case, turn to this article and use these steps in making a patient medical report.
Who Writes the Patient Medical Report?
Health care providers do the patient medical report. The health care professionals make the documentation for a patient. It includes all the physicians, nurses, and doctors of medicine. It also includes the psychiatrists, pharmacists, midwives and other employees in the allied health.
Who Can Have Access to a Patient Medical Report?
The health care providers have the access to the patient medical report. They keep the medical report as a history of medical records. Also, patients’ access to the patient medical report is a must. It is their right to see their medical report. It is against the law not to show them their medical report.
Is a Patient Medical Report a Legal Document?
If it is signed by a health care professional, then it is a legal document. It is permissible in any court of law. It is an evidence that the patient is under your care. Thus, it can be used in court as an essential proof. So, keep a patient medical report because you may need it in the future.
How to sign a patient care report on iPhone?
To sign a patient care report template doc right from your iPhone or iPad, just follow these brief guidelines: Install the signNow application on your iOS device. Create an account using your email or sign in via Google or Facebook. Upload the PDF you need to e-sign.
What is the purpose of PCR?
The primary purpose of the Patient Care Report (PCR) is to document all care and pertinent patient information as well as serving as a data collection tool.
You Need a Nursing Brain Sheet That Works for YOU
For the longest time I have tried pushing the brain sheet that worked for me onto new students and newbie nurses. I’ve changed my tone.
The Nursing Brain Sheet Database
The response was AMAZING (to say the least). We received over 100 report sheet templates from nurses working in MedSurg, ICU, ED, OB, Peds, Tele . . . you name it.
1. Handoff and Nursing Report Sheet
This is the report sheet that my preceptor used to make me fill out prior to the end of each shift as a newbie. To be honest, at first I was so annoyed that I had to spend like an hour at the end of each shift filling this out. It wasn’t until I realized I was able to give a badass report that I was finally grateful she made me fill this out.
3. 4 Patient Simple Tele Sheet
Some people like it simple . . .this is the sheet for you. With slight prompting this sheet makes a great tool for the MedSurg or Tele nurse on the GO!
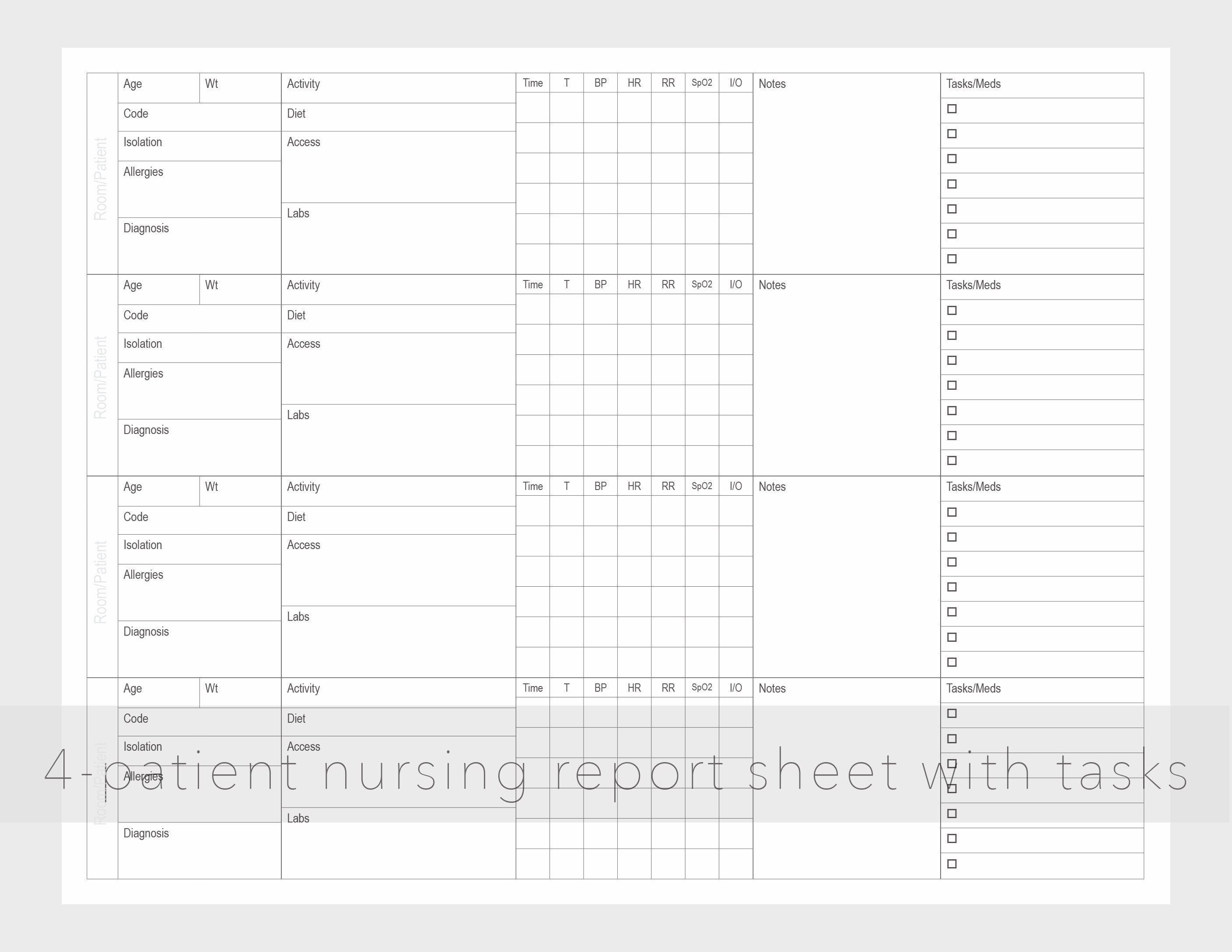
4. 4 Patient Simple Nurse Task Sheet
I love this one. At first glance it looks basic . . . put at closer inspection you start to see all the details and information you have available with it. From lab values, to foley care, to last pain med, this is would be a great one for a nurse that has a flow and just wants a simple push to stay a bit more organized.
5. Vertical Nurse Brain sheet with Assessment Diagram
I’m a visual learner. This one just grabs my attention. I like the top section for the “essentials” like blood sugars, DX, and Pt info. I also really like the area below the charts to draw little notes about your physical assessment. I really like this nursing brain sheet for beginner or experience nurse.
6. Just the Boxes
I’ll be honest . . . after a couple years of being a nurse my “brainsheet” has evolved into more of a few freehand drawing on a sheet of paper. If that sounds like you, this is probably the one for you. With little more than a few suggestions . . . this is a pretty basic organizer for nurses.
What is a nursing report sheet?
Nursing report sheets are premade templates of paper used by nurses to help them keep track of their patients. A nursing report sheet is started at the beginning of the nurses shift while she/he is getting report from the leaving nurse who is giving them nursing report.
What is a nursing note?
Nursing notes to remind yourself of things you need to do for the patient or chart on. Notes to yourself on things you want to remind the next shift. Most nurses who use report sheets consider their report sheet to be their “brain,” and panic when they misplace them.
Why do nurses use report sheets?
Why Do Nurses Use Nursing Report Sheets? Nurse report sheets are very handy because they contain tidbits of vital information concerning your patient’s diagnosis, history, allergies, attending doctor,consults, things that need to be done on your shift, medication times, vital signs, lab results etc. The report sheet has other usage as well.
Why is it important to have a 6 to 7 patient load?
When you have a 6 to 7 patient load, patient diagnosis and histories can run together and you may get them confused. Helps you keep your charting more accurate. If you write down on your report sheet things you need to remember to chart, your charting will be more accurate and easier to do.
Can you print a report sheet for nurses?
You can share them with other nurses as well. Simply click the picture of the report sheet you like and after you download it you can print them. Tip: for less report sheets to carry around set your printer settings so you can print on the back side.
What are the different types of medical reports?
Types of Medical Report Templates 1 Patient Medical Report Example – This is what you need if you’re looking for a generic medical report template. This medical report targets any patient with certain illnesses, ideal for clinic or hospital use. This contains needed information such as patient’s complete name, address, contact details, questions about medical status/history, and other related medical questions. 2 Hospital Medical Report Template – This type of medical report is designed for hospital use. Information includes patient’s name, ward, hospital name, medical consultant, discharge summary, the reason for admission and medical diagnosis, and past medical history. 3 Medical Examination Report Example – If you’re making medical reports intended for medical examinations, perhaps you might want to download this template for more convenience. This is a complete template that targets examination reports in a medical setting. 4 Medical Incident Report Template – This type of medical report focuses on any incident or accident that may happen within a medical setting. This is filled so that recording of details about incidents that occur at the medical facility will be tracked down and certain measures or sanctions will be implemented. 5 Medical Fitness Report Template – Making medical reports for fitness progress? This template is what you need. This aims at providing a thorough and complete report for medical fitness. The template contains information such as applicant’s name, address, license number, name of the hospital/clinic who conducted the report, and questions related to medical fitness.
Why is it important to update medical reports?
In every patient’s life, change always comes, may it be a changed name, address, medical progress, or a new health diagnosis and prescription.
What should be written down in a medical history?
Effects of alcohol, intellectual, emotional, psychiatric, and other drugs taken should be written down. Regardless if there are negative findings, it should also be included. Medical History. When writing a patient’s medical history, relevant medical conditions should be considered.
What forms are used to bill and reimburse?
Other medical forms include medical invoices, which both bill and reimburse individuals for health services they may have received, as well as medical records and logs , which document health concerns or issues, record medical history and records, and monitor medication schedules or recurring illnesses.
What is a medical trial plan?
Document, track, and manage a medical or clinical trial plan with this comprehensive template. List each step of the process, including start-up, ongoing, and close-out activities. With space to record safety plans and procedures, protocol developments, and clinical study reports and reviews, this document helps to manage all aspects of a medical procedure or trial.
Outline
Providing a concise nursing report allows for greater continuity of care.
Transcript
Providing a clear and concise nursing report is an art form that allows for greater continuity of care. In this lesson, we’re going to discuss a method for gathering and reporting on patient data in a uniform way that ensures clarity.

Popular Posts:
- 1. uw health odana clinic patient portal
- 2. a patient with ckd lad report
- 3. fairlawn dermatology patient portal
- 4. va cancer institute patient portal
- 5. robinson uh patient portal setup
- 6. phoenix health patient portal
- 7. patient portal follow my health pih
- 8. forest county potawatomi community patient portal
- 9. lewis gale patient portal
- 10. gotham gastro patient portal