Patient Care Report (PCR) - Appropedia: The …
5 hours ago General information on a patient care report will not get you anywhere. In this kind of field, being more specific especially with the diagnosis and the status of the patient is better than just stating the patient is okay. So when you are writing your PCR or patient care report, why don’t you try and be more specific. It makes all the difference. 2. >> Go To The Portal
Do you need to complete a patient care report (PCR)?
We can all agree that completing a patient care report (PCR) may not be the highlight of your shift. But it is one of the most important skills you will use during your shift.
What are prehospital care reports (PCRs)?
Re: Prehospital Care Reports (PCRs) Page 1 of 5 Documentation is an essential part of all prehospital medical care. It must include, but not be limited to the documentation of the event or incident, the medical condition, treatment provided and the patient’s medical history.
What is PCR documentation in the medical field?
The PCR documentation is considered a medical document that becomes part of the patient’s permanent medical record. It is also considered a legal document in cases where liability and/or malpractice issues arise. It is the source in which all medical billing claims are based.
Who can enter information on the PCR/EPCR?
Policy Statement 12-02 Page 1 of 5 Information Entry: All information written on the paper PCR should be legible and printed in blue or black ink. Any member of the crew may enter information on the PCR/ePCR. The individual indicated as “In Charge” should be the person who provided or directed the care to the patient.
What is a PCR report?
PCR means polymerase chain reaction. It's a test to detect genetic material from a specific organism, such as a virus. The test detects the presence of a virus if you have the virus at the time of the test. The test could also detect fragments of the virus even after you are no longer infected.
How do I write a PCR report?
Follow these 7 Elements to Paint a Complete PCR PictureDispatch & Response Summary. ... Scene Summary. ... HPI/Physical Exam. ... Interventions. ... Status Change. ... Safety Summary. ... Disposition.
What should a patient care report include?
What Patient Care Reports Should IncludePresenting medical condition and narrative.Past medical history.Current medications.Clinical signs and mechanism of injury.Presumptive diagnosis and treatments administered.Patient demographics.Dates and time stamps.Signatures of EMS personnel and patient.More items...•
What information is patient data on a PCR?
What is a primary difference in the type of information found in the administrative section and in the patient information section of the PCR? A. The patient information includes the patient's address only and the administrative section includes the trip times.
How do you write a patient assessment?
Assessment & PlanWrite an effective problem statement.Write out a detailed list of problems. From history, physical exam, vitals, labs, radiology, any studies or procedures done, microbiology write out a list of problems or impressions.Combine problems.
What can you record on a PCR?
This includes the agency name, unit number, date, times, run or call number, crew members' names, licensure levels, and numbers. Remember -- the times that you record must match the dispatcher's times.
What the patient care report represents?
Patient care report or “PCR” means a computerized or written report that documents the assessment and management of the patient by the emergency care provider in the out-of-hospital setting. “ Pharmacy-based” means that ownership of the drugs maintained in and used by the service program.
What clinical patient information is included in the Minimum data Set on a PCR?
MINIMUM DATA SET: two separate types of data that are recorded,PATIENT INFORMATION: chief complaint, the initial assessment, vital signs, and. patient demographics.ADMINISTRATIVE INFORMATION: the time the incident was reported, the time the responding unit was notified, the time of arrival at the patient,
How do I give a good report in EMS?
There are several things that go into giving an effective HEAR report....It should include:Who you are.Coming in emergently or non-emergently.How far away you are.Age of patient.Type of patient you are bringing.The patient's chief complaint.What you have done for the patient.Patient's vital signs.
Who is responsible for documenting details about a patient's treatment and transport in the PCR?
Upon delivery of the patient in the medical facility, under ideal circumstances the EMT will complete a full PCR containing all of the patients data, obtain a transfer-of-care signature from the medical professional who is assuming responsibility, and leave a copy of the full report with the facility.
What is an objective patient assessment finding?
Examples of objective assessment include observing a client's gait , physically feeling a lump on client's leg, listening to a client's heart, tapping on the body to elicit sounds, as well as collecting or reviewing laboratory and diagnostic tests such as blood tests, urine tests, X-ray etc.
What is the difference between the patient information section of the PCR and the administrative information that is included on the PCR?
What is the difference between the patient information section of the PCR and the administrative information that is included on the PCR? The patient information includes specific assessment findings, and the administrative information includes the trip times.
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the inf...
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very caref...
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make...
What Is a Patient Care Report?
We often hear of care reports based on by medical teams or by medical authorities. Yet, we are not sure how this differs from the kind of report that is given to us by the same people. So this is the time to make it as clear as possible.
How to Write a Patient Care Report?
Where do you even begin when you write a patient care report? A lot of EMS or EMTs do know how to write one since they are trained to do so.
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the information necessary for the assessment and evaluation of a patient’s care.
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very careful and very meticulous when writing these kinds of reports. Every detail counts.
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make sure that you have all the information correctly. One wrong information can cause a lot of issues and problems.
How to Edit Your Ems Pcr Template Pdf Form Online
When you edit your document, you may need to add text, fill in the date, and do other editing. CocoDoc makes it very easy to edit your form with the handy design. Let's see how to finish your work quickly.
How to Edit Text for Your Ems Pcr Template Pdf Form with Adobe DC on Windows
Adobe DC on Windows is a popular tool to edit your file on a PC. This is especially useful when you finish the job about file edit without using a browser. So, let'get started.
How to Edit Your Ems Pcr Template Pdf Form With Adobe Dc on Mac
Find the intended file to be edited and Open it with the Adobe DC for Mac.
How to Edit your Ems Pcr Template Pdf Form from G Suite with CocoDoc
Like using G Suite for your work to sign a form? You can make changes to you form in Google Drive with CocoDoc, so you can fill out your PDF without worrying about the increased workload.
What is PCR in healthcare?
The PCR must paint a picture of what happened during a call. The PCR serves: 1 As a medical record for the patient, 2 As a legal record for the events that took place on the call, and 3 To ensure quality patient care across the service.
What should a PCR tell?
The PCR should tell a story; the reader should be able to imagine themselves on the scene of the call.
Why is PCR important?
A complete and accurate PCR is essential for obtaining proper reimbursement for our ambulance service, and helps pay the bills, keeps the lights on and the wheels turning. The following five easy tips can help you write a better PCR: 1. Be specific.
Why do you write PCR when you call?
Writing the PCR as soon as the call is over helps because the call is still fresh in your mind . This will help you to better describe the scene and the condition the patient was in during your call.
How long does it take to complete a PCR?
Most states, and many EMS agencies themselves, often have time limits within which the PCR must be completed after the call ended – 24, 48 or 72 hours are common time limits.
Why is an IV established on the patient?
This specifically explains why an IV was established on the patient and states facts that can be used to show medical necessity for the call. The same can be said for non-emergency transports between two hospitals. Simply documenting that the patient was transported for a “higher level of care” is not good enough.
How to determine if a medical necessity is met?
A primary way to determine if medical necessity requirements are met is with documentation that specifically states why you took the actions you did on a call. For example, simply documenting “per protocol” as the reason why an IV was started or the patient was placed on a cardiac monitor is not enough.
What is a PCR/EPCR?
The PCR/ePCR may also serve as a document called upon in legal proceedings relating to a person or an incident. No EMS agency is obligated to provide a copy of the PCR/ePCR simply at the request of a law enforcement or other agency. If a copy of the PCR/ePCR is being requested as part of an official investigation the requestor must produce either a subpoena, from a court having competent jurisdiction, or a signed release from the patient. PCR/ePCR must be made available for inspection to properly identified employees of the NYS Department of Health.
How often do you submit PCRs for ambulance?
PCRs shall be submitted at least monthly, or more often if so indicated by the program agency.
What is the confidentiality of health information?
Maintaining confidentiality is an essential part of all health care, including prehospital care. The confidentiality of personal health information (PHI) is covered by numerous state and federal statutes, Polices, Rules and Regulations, including the Health Insurance Portability & Accountability Act of 1996 (HIPAA) and 10 NYCRR.
Do EMS have to leave PCR?
EMS services are required to leave a paper copy or transfer the electronic PCR information to the hospital prior to the EMS service leaving the hospital. This document must minimally include, patient demographics, presenting problem, assessment findings, vital signs, and treatment rendered.

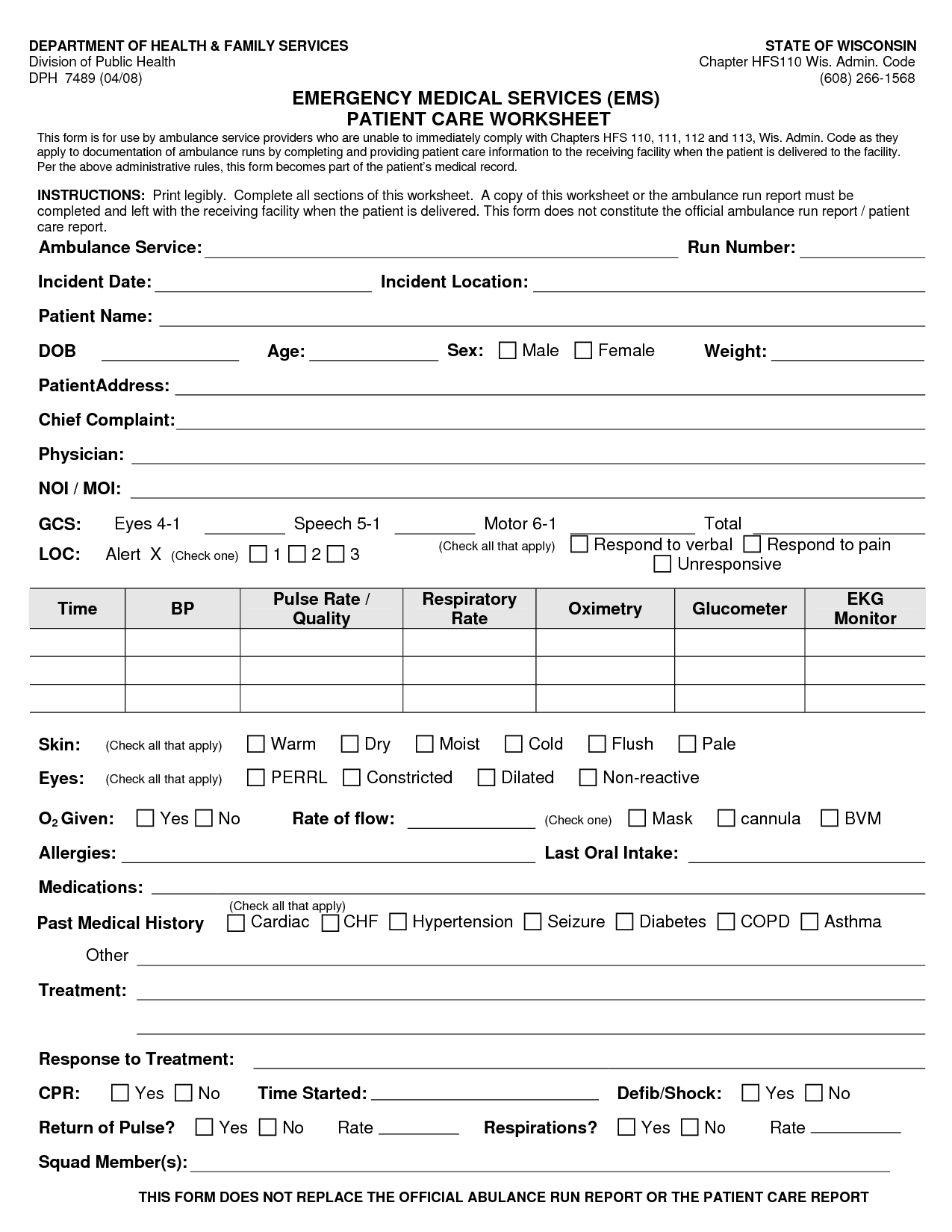
Structure
- The EMS PCR record should include: 1. Patient demographics such as name, address, date of birth, age, and gender. 2. Dispatch data, such as the location of the call and times related to the call such as time on scene for rescuers and first responders. 3. Provider's initial impression of the patient and the scene including details on the mechanism o...
Format and Execution
- These records may be organized in many different formats. Many agencies use pre-printed standardized forms with both check boxes and areas for narrative descriptions for hand written documents, or mobile electronic data entry systems for feeding data directly into integrated Electronic Health Records (EHRs). Whatever the format, the PCR is only as good as the informati…
Legal Aspects
- Thorough PCRs help support the medical diagnosis, provide a rationale for treatment decisions in the field, and demonstrate that responders adhered to their local protocols. Complete documentation is the best defense should there ever be litigation around a poor outcome. Negligence Failure to document can lead to questions regarding the appropriateness of care, an…
Special Reporting Situations
- As an EMT in the US you are a mandated reporterfor child/adult/elder abuse. This means that you are legally obliged to make a report to Child/Adult Protective Services if you believe on reasonable grounds that a child is in need of protection from physical injury or sexual abuse, and to make the report as soon as practicable after forming your belief. Other situations such as incidents involvi…
Tips and Tricks
- Limit potential perjury. The PCR is a legal document, so stating that a patient is GCS 15 when you state that they are confused earlier on is technically lying and could be used to undermine your P...
- Mistakes in charting commonly occur in situations where the provider routinely contacts similar patients (i.e. most urban EMS systems). Not every patient is critical, or even requires …
- Limit potential perjury. The PCR is a legal document, so stating that a patient is GCS 15 when you state that they are confused earlier on is technically lying and could be used to undermine your P...
- Mistakes in charting commonly occur in situations where the provider routinely contacts similar patients (i.e. most urban EMS systems). Not every patient is critical, or even requires ambulance tra...