Nursing Report Sheet Template: 15 Best Templates and …
32 hours ago Med-Surg Telemetry Nurse Brain (3 patients per sheet) TheBohoNurse. (1) $2.85. Four Patient Nurse Report Sheet template. SBAR RN Handoff. Simple full patient assessment. Med Surg … >> Go To The Portal
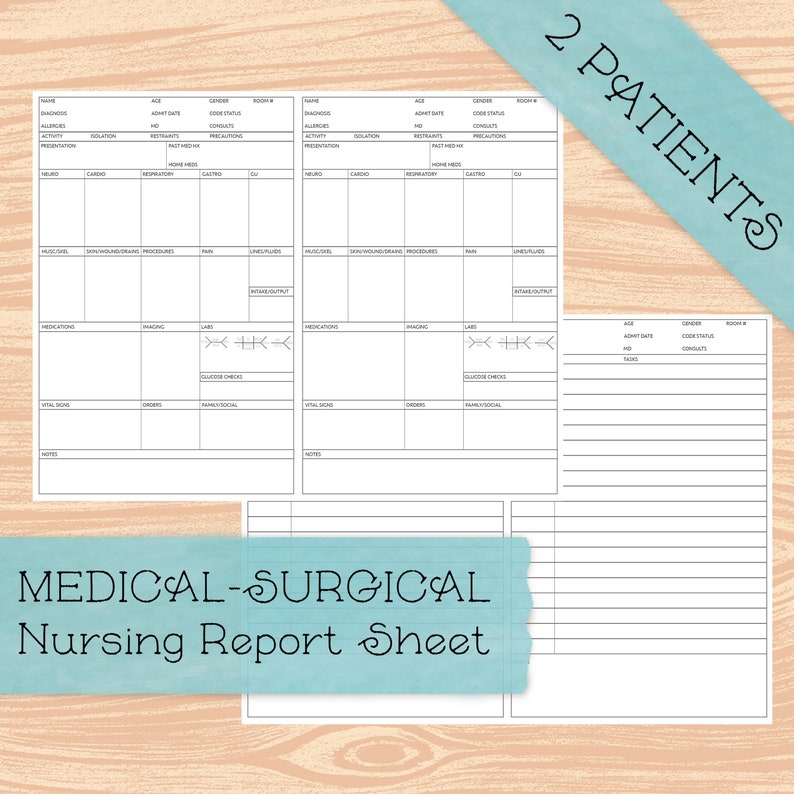
What is a nursing report sheet? Nursing report sheets, also known as patient report sheets or a nursing brain sheet, are templates nurses fill out with important patient information. These sheets are handoffs at the end of each shift and are given to the new nurse taking over for the next shift.
Full Answer
What are nurses required to report?
The law requires nursing homes to disclose more detailed financial information. This is especially important as an increasing number of facilities are owned by private equity firms. The law imposes additional requirements on facilities with repeated code violations, including more frequent surveys and more stringent penalties.
Can a nurse refuse treatment of a patient?
You cannot refuse to be involved in the care of patients because of their condition or the nature of their health problems. All blood and body fluids should be treated as infectious. All health care staff should understand local and national standards for infection control precautions. Please also see our infection protection and control guidance .
How do nurses affect patient outcomes?
“As a key player on the front lines of health care delivery, nurses play a critical role in preventing adverse events, coordinating care and enabling patients to achieve optimal outcomes,” Press Ganey states.
Should nurse to patient ratios be mandated?
The bill mandates that a one-to-one nurse-patient ratio would be imposed for patients in the ICU, OR, trauma, critical care, as well as for unstable neonates and patients needing resuscitation. Another provision of the bill places a one-to-three nurse-patient ratio limit for pediatrics and patients who are pregnant.
How do you write a nurse report sheet?
0:0020:45Nursing Shift Report Sheet Templates | How to Give a Nursing Shift ReportYouTubeStart of suggested clipEnd of suggested clipSo to get that you can go to our website registered nurse RN comm. Go to the search bar which is atMoreSo to get that you can go to our website registered nurse RN comm. Go to the search bar which is at the top right and type nursing report templates or nursing report sheets.
How should a nurse write a patient report?
How to write a nursing progress noteGather subjective evidence. After you record the date, time and both you and your patient's name, begin your nursing progress note by requesting information from the patient. ... Record objective information. ... Record your assessment. ... Detail a care plan. ... Include your interventions.
What should be included in a nurse to nurse report?
What to cover in your nurse-to-nurse handoff reportThe patient's name and age.The patient's code status.Any isolation precautions.The patient's admitting diagnosis, including the most relevant parts of their history and other diagnoses.Important or abnormal findings for all body systems:More items...•
What is a nursing brain sheet?
A "brain sheet" is simply a reference used by nurses so they can keep track of important information about each patient. This sheet is often filled out with key information during change-of-shift report and then updated as things change (and they always do!).
How do you write a patient report?
Summary: The format of a patient case report encompasses the following five sections: an abstract, an introduction and objective that contain a literature review, a description of the case report, a discussion that includes a detailed explanation of the literature review, a summary of the case, and a conclusion.
How do I fill out a patient care report?
There are seven elements (at a minimum) that we have identified as essential components to documenting a well written and complete narrative.Dispatch & Response Summary. ... Scene Summary. ... HPI/Physical Exam. ... Interventions. ... Status Change. ... Safety Summary. ... Disposition.
How do you do nursing documentation?
Nursing Documentation TipsBe Accurate. Write down information accurately in real-time. ... Avoid Late Entries. ... Prioritize Legibility. ... Use the Right Tools. ... Follow Policy on Abbreviations. ... Document Physician Consultations. ... Chart the Symptom and the Treatment. ... Avoid Opinions and Hearsay.More items...
What should be included in nursing progress notes?
3:5114:49What you need to know about writing a progress note (Nursing School ...YouTubeStart of suggested clipEnd of suggested clipThe most important takeaway here is that you want to document the things that happen because if youMoreThe most important takeaway here is that you want to document the things that happen because if you don't it didn't happen so did a lot of different ways to write a progress note however will discuss
What are the types of nursing documentation?
The most common types of nursing documentation include the following:Nursing Progress Notes.Narrative Nursing Notes.Problem-Oriented Nursing Notes.Charting By Exception Nursing Notes.Nursing Admission Assessment.Nursing Care Plans.Graphic Sheets.Medication Administration Records (MARs)
What is a nurse report?
Nursing report is given at the end of the nurses shift to another nurse that will be taking over care for that particular patient. Nursing report is usually given in a location where other people can not hear due to patient privacy.
How do you use a nursing brain sheet?
0:227:33Nurse Brain Sheet | Organize Report For Your Nurse Shift || TriciaYsabelleYouTubeStart of suggested clipEnd of suggested clipWrite their notes down for the shift. Including their assessment times any important tasks that theyMoreWrite their notes down for the shift. Including their assessment times any important tasks that they have to any meds that they need to give. So if you see nurses walking around.
What do neuroscience nurses do?
A Neuroscience Nurse helps patients who experience brain and nervous system disorders, such as Alzheimer's, strokes, and brain injuries, recover from or learn to manage their condition.
Does Etsy offer free shipping?
Shipping policies vary, but many of our sellers offer free shipping when you purchase from them. Typically, orders of $35 USD or more (within the s...
How do I personalize items on Etsy?
Found something you love but want to make it even more uniquely you? Good news! Many sellers on Etsy offer personalized, made-to-order items. To pe...
Does shopping on Etsy help support small businesses?
Absolutely! Our global marketplace is a vibrant community of real people connecting over special goods. With powerful tools and services, along wit...
Are the products on Etsy handmade?
From handmade pieces to vintage treasures ready to be loved again, Etsy is the global marketplace for unique and creative goods. It’s also home to...
What is a nursing report sheet?
Nursing report sheets are premade templates of paper used by nurses to help them keep track of their patients. A nursing report sheet is started at the beginning of the nurses shift while she/he is getting report from the leaving nurse who is giving them nursing report.
Why do nurses use report sheets?
Why Do Nurses Use Nursing Report Sheets? Nurse report sheets are very handy because they contain tidbits of vital information concerning your patient’s diagnosis, history, allergies, attending doctor,consults, things that need to be done on your shift, medication times, vital signs, lab results etc. The report sheet has other usage as well.
What is a nursing note?
Nursing notes to remind yourself of things you need to do for the patient or chart on. Notes to yourself on things you want to remind the next shift. Most nurses who use report sheets consider their report sheet to be their “brain,” and panic when they misplace them.
Why is it important to have a 6 to 7 patient load?
When you have a 6 to 7 patient load, patient diagnosis and histories can run together and you may get them confused. Helps you keep your charting more accurate. If you write down on your report sheet things you need to remember to chart, your charting will be more accurate and easier to do.
Can you print a report sheet for nurses?
You can share them with other nurses as well. Simply click the picture of the report sheet you like and after you download it you can print them. Tip: for less report sheets to carry around set your printer settings so you can print on the back side.
What is a nursing report sheet?
A nurse report sheet, also referred to as a nursing brain sheet, is a piece of paper that contains organized information on your patients. The sheets will look differently depending on what specialty you work in at the hospital. Some of the information on a nursing brain ...
Why do hospitals use electronic charting software?
Computer charting software is essential so that patients’ medical information is in one place.
Is paperless charting good for nurses?
But even with substantial technological advances in paperless charting, it is still beneficial for nurses to keep essential information at their fingertips. This is where a nursing report sheet comes to play.
You Need a Nursing Brain Sheet That Works for YOU
For the longest time I have tried pushing the brain sheet that worked for me onto new students and newbie nurses. I’ve changed my tone.
The Nursing Brain Sheet Database
The response was AMAZING (to say the least). We received over 100 report sheet templates from nurses working in MedSurg, ICU, ED, OB, Peds, Tele . . . you name it.
1. Handoff and Nursing Report Sheet
This is the report sheet that my preceptor used to make me fill out prior to the end of each shift as a newbie. To be honest, at first I was so annoyed that I had to spend like an hour at the end of each shift filling this out. It wasn’t until I realized I was able to give a badass report that I was finally grateful she made me fill this out.
3. 4 Patient Simple Tele Sheet
Some people like it simple . . .this is the sheet for you. With slight prompting this sheet makes a great tool for the MedSurg or Tele nurse on the GO!
4. 4 Patient Simple Nurse Task Sheet
I love this one. At first glance it looks basic . . . put at closer inspection you start to see all the details and information you have available with it. From lab values, to foley care, to last pain med, this is would be a great one for a nurse that has a flow and just wants a simple push to stay a bit more organized.
5. Vertical Nurse Brain sheet with Assessment Diagram
I’m a visual learner. This one just grabs my attention. I like the top section for the “essentials” like blood sugars, DX, and Pt info. I also really like the area below the charts to draw little notes about your physical assessment. I really like this nursing brain sheet for beginner or experience nurse.
6. Just the Boxes
I’ll be honest . . . after a couple years of being a nurse my “brainsheet” has evolved into more of a few freehand drawing on a sheet of paper. If that sounds like you, this is probably the one for you. With little more than a few suggestions . . . this is a pretty basic organizer for nurses.
What is a nursing report?
A nursing report focuses on providing accurate details of nursing by developing conducted research understood to the complete level of practicing nurses, educators, and interested members of the public. The sample report templates act as a huge help when it comes to constructing a precise nursing report. You may also check here Report Examples
What is included in a clinical report?
Any relevant clinical information is also included such as a change in condition, adverse findings or events, patient outcomes, clinical investigations, and other relevant aspects. Don’t forget to close the report with companion documents. These are patient identification, nursing assessment, and legislative compliance.
Why is it important to have a nursing report?
It is important for good clinical communication to have a concise nursing report. A great report provides an accurate reflection of nursing assessments to support the medical team to provide great care. Objective. To provide a structured and standardized approach regarding nursing report and documentation.
How to make a good decision in a report?
Support your decision with statistics and facts. As much as possible, keep your report short and concise. The shorter the better. You need to summarize your message and write it down on the first page. Make sure to keep the body of your report as short as possible.
