7+ Patient Chart Templates – DOC, PDF, Excel
3 hours ago A lot of people believe that only nurses or health care workers can write reports.Most specifically patient care reports or anything that may be related to an incident report that often happens in hospitals or in some health care facilities. It would seem that when you hear the words patient and care with the word report mixed to it, you would immediately think, oh nurses are mostly … >> Go To The Portal
What is a patient chart template?
A patient chart is an important tool to track the health or medical record of a patient. These Medication Chart Templates are designed as systematical accounts of the medical history & care received by a patient by one specific doctor or say hospital.
What does a patient care report consist of?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the information necessary for the assessment and evaluation of a patient’s care. What should not be written in a patient care report?
What is a hospital patient chart in Canada?
health.gov.nl.ca | The hospital patient chart is a comprehensive chart which records every minute information required for diagnosis. It also wants to know about previous medications, allergies and operations that the patient might have had.
What are the different types of patient care templates?
When you download one of these top patient care templates, you’ll find a wide variety of options from care plan template for learning disability to care plan template for the elderly. There are templates that come as care plan templates for schools, care plan templates for residential homes and even care plan templates for children.
How do you write a patient care report?
There are seven elements (at a minimum) that we have identified as essential components to documenting a well written and complete narrative.Dispatch & Response Summary. ... Scene Summary. ... HPI/Physical Exam. ... Interventions. ... Status Change. ... Safety Summary. ... Disposition.
How do you write a good PCR?
How to Write an Effective ePCR NarrativeBe concise but detailed. Be descriptive in explaining exactly what happened and include the decision-making process that led to the action. ... Present the facts in clear, objective language. ... Eliminate incorrect grammar and other avoidable mistakes. ... Be consistent and thorough.
What is EMS chart?
CHART stands for Chief Complaint History Assessment Received Treatment Transfer of Care (Emergency Medical Care Narrative for Reporting) Suggest new definition.
What does the R stand for in chart documentation?
C.H.A.R.T. C = Chief Complaint. H = History (Past & Present) A = Assessment. R = Rx or Treatment.
What is a PCR in writing?
The PARCC Summative Assessments in Grades 3-11 will measure writing using three prose constructed response (PCR) items. In the classroom writing can take many forms, including both informal and formal.
What is a PCR document?
The PCR documentation is considered a medical document that becomes part of the patient's permanent medical record. It is also considered a legal document in cases where liability and/or malpractice issues arise. It is the source in which all medical billing claims are based.
What is the chart method?
The charting method is a note-taking method that uses charts to condense and organize notes. It involves splitting a document into several columns and rows which are then filled with summaries of information. This results in a note format that enables efficient comparisons between different topics and ideas.
How do you make a narrative chart?
CHART narratives also follow a visual layout based on the letters in the acronym. Starting with the chief Complaint, the History of the present illness, along with the patient's past medical history, are outlined. Assessment findings are then documented, along with Rx (prescriptions) that the patient is prescribed.
What does the A in chart stand for?
Definition. CHART. Coordinated Highways Action Response Team. CHART.
What are the 6 C of charting?
Client's Words, Clarity, Completeness, Conciseness, Chronological Order and Confidentiality.
What does D mean on medical records?
every. q.1.d., q1d. every day. q.1.h., q1h. every hour.
What does PB stand for in medical terms?
Abbreviation for phenobarbital; symbol for lead (plumbum).
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the inf...
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very caref...
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make...
What is patient chart template?
A patient chart template sample enables the doctors or caregivers to instantly understand whether the patient is progressing or deteriorating under the present care. These Chart Templates serves a great role in helping the doctor to decide the steps or doses for further treatment.
What is hospital patient chart?
health.gov.nl.ca | The hospital patient chart is a comprehensive chart which records every minute information required for diagnosis. It also wants to know about previous medications, allergies and operations that the patient might have had.
What is a dental patient chart sample?
The dental patient chart sample is a comprehensive chart that requires a lot of information for diagnosis. The sample is a dental chart for dogs. It asks the general information of the pet and also records the procedures.
What is a patient observation chart?
library.nhsggc.org.uk | The patient observation chart is a comprehensive which takes all the required information of the patient. It also has the guidelines and a pain score and a sedation score for the patient.
What is an inpatient drug chart?
connect.qualityincare.org | The inpatient drug chart is for all the patients admitted to hospitals and rehabs. It contains the general information about the patient and also records the drugs administered and the side effects of the drug.
What Is a Patient Care Report?
We often hear of care reports based on by medical teams or by medical authorities. Yet, we are not sure how this differs from the kind of report that is given to us by the same people. So this is the time to make it as clear as possible.
How to Write a Patient Care Report?
Where do you even begin when you write a patient care report? A lot of EMS or EMTs do know how to write one since they are trained to do so.
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the information necessary for the assessment and evaluation of a patient’s care.
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very careful and very meticulous when writing these kinds of reports. Every detail counts.
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make sure that you have all the information correctly. One wrong information can cause a lot of issues and problems.
What is a patient care plan template?
The Patient Care Plan Template is a document that mentions almost everything that a patient and the family need to do in order to ensure faster recovery of the impacted person. Following a proper routine or detailed chart for the entire day helps the patient to stay relaxed and ensure that he/she only eat, perform, or rest as per the mentioned timelines for recovering fast. You may also see Child Care Plan Template.
What is a care plan for patients with complex needs?
The Care Plans for Patients with Complex Needs Template is used by most of the hospitals, nursing homes, clinics, and medical institutions provide detailed care plans to patients when they get discharged. All of these plans and procedures aim at ensuring optimal health, and speedy recovery of the patient, even if they leave from the medical institution from where their treatment was going on. You may also see Editable Daycare Business Plan Templates.
What is a mental health treatment plan?
The Mental Health Treatment Plan templates are being used by the patient or by the health professional to ensure that correct medication, diet, and routine has been followed during their treatment process.
How to Edit Your Ems Pcr Template Pdf Form Online
When you edit your document, you may need to add text, fill in the date, and do other editing. CocoDoc makes it very easy to edit your form with the handy design. Let's see how to finish your work quickly.
How to Edit Text for Your Ems Pcr Template Pdf Form with Adobe DC on Windows
Adobe DC on Windows is a popular tool to edit your file on a PC. This is especially useful when you finish the job about file edit without using a browser. So, let'get started.
How to Edit Your Ems Pcr Template Pdf Form With Adobe Dc on Mac
Find the intended file to be edited and Open it with the Adobe DC for Mac.
How to Edit your Ems Pcr Template Pdf Form from G Suite with CocoDoc
Like using G Suite for your work to sign a form? You can make changes to you form in Google Drive with CocoDoc, so you can fill out your PDF without worrying about the increased workload.
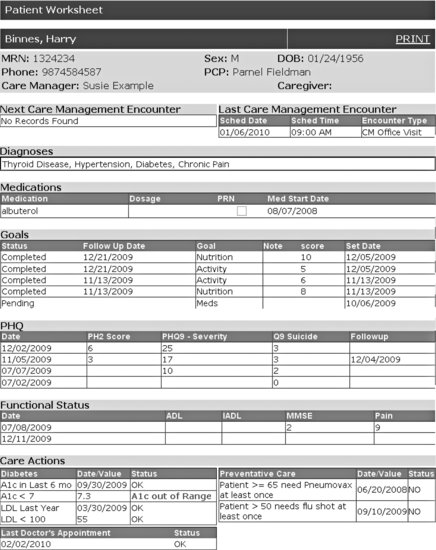
What is a nursing report sheet?
The report sheets enable the nurses to record clear information regarding details including the diagnosis, history, allergies, consults, vital signs, lab results, and other such health-related data. Due to their excellent recording system, nursing report sheets are used by physicians, doctors, nurses and other healthcare staff all over the world. ...
What is reporting in nursing?
In medical circles, reporting refers to the act of transferring relevant information. In most cases, this information refers to the patient information that is transferred from one nurse to another during the change of shift. There are numerous occasions that require reporting.
Why is a mental health nursing report important?
It allows nurses and doctors to continue treating and providing care to their patients even when during shift interchange.
Why is it important to have an ICU nurse report?
Due to this, it is very important that nurses are able to gather the required information. To help with this situation, ICU Nursing Reports were brought into action. ICU Nursing Reports are used to obtain a list of essential details regarding the patient who has been admitted to the ICU.
Why do nurses use advance notes?
Advance notes to prompt nurses about the duties that they need to perform in the next shift. Moreover, nursing report sheets play a huge role in favor of the nurse’s life as well. Due to the vast expanse of the information present, a lot of nurses consider the reports to be akin to a secondary brain.
What is the purpose of the General Information section in a nursing report?
This section is responsible for generating all the details regarding the patient such as Date of Birth, Gender etc. of the patient.
What is flow sheet in nursing?
A6. In simple terms, a flow sheet is a single or dual-page form, tasked with the job of gathering all important aspects of a patient’s condition. Similar to the other nursing reports, the flow sheet is tasked with gathering patient information.