Nursing Report Sheet Template: 15 Best Templates and …
2 hours ago Structure & sample of nursing shift change report sheet. 5b21e1456b55a.php. Image Courtesy – Registered Nurse RN . ... If you find any confusion, then ask and not simply fill the form. Try to check the patient’s basic details like name, age, etc before you continue to fill the form. >> Go To The Portal
What is a nurses shift report sheet?
Nurse Shift Report Sheets are not not an uncommon occurrence at healthcare institutions. They are often viewed as a crucial entity that helps them to pass on patient information during routine changes in the shifts of nurses.
What is a med surg organization sheet?
For example, the room where the patient was treated, the name of the patient, the contact of the person closest to the patient, the condition of the patient during treatment, and also the type of care received. Med surg organization sheet functions as a journal report. So that tracking can be done in patients who have just had surgery.
Who can use the shift change report?
You can understand this information to effectively use the shift change report. Hospitals, nursing homes, medical health care providers, and individual nurses can use this sheet for effective communication about the patient. We can understand your concern and would like to clarify.
What is a med surg nurse?
What is the Med Surg department? Med Surg is part of the medical department. Med Surg stands for medical-surgical which is a department that contains nurses specifically handling patients who need recovery after undergoing surgery. There is no specific age for patients treated by Med Surg nurses.
What should a nurse shift report include?
It should include the patient's medical history, current medication, allergies, pain levels and pain management plan, and discharge instructions. Providing these sorts of details about your patient in your end of shift report decreases the risk of an oncoming nurse putting the patient in danger.
How do you write a shift report?
Tips for an Effective End-of-Shift ReportUse Concise and Specific Language. ... Record Everything. ... Conduct Bedside Reporting as Often as Possible. ... Reserve Time to Answer Questions. ... Review Orders. ... Prioritize Organization. ... The PACE Format. ... Head to Toe.
How do I write a nursing daily report?
How to write a nursing progress noteGather subjective evidence. After you record the date, time and both you and your patient's name, begin your nursing progress note by requesting information from the patient. ... Record objective information. ... Record your assessment. ... Detail a care plan. ... Include your interventions.
How do you organize a nursing report sheet?
0:1210:04Nurse Brain Sheet | ORGANIZE YOUR NURSING SHIFT | Nursing ReportYouTubeStart of suggested clipEnd of suggested clipOrganization tips for you to be successful during your nursing shift the main one being a reportMoreOrganization tips for you to be successful during your nursing shift the main one being a report sheet and this is what people call their nurse brains.
How do you write a patient report?
III. Patient case presentationDescribe the case in a narrative form.Provide patient demographics (age, sex, height, weight, race, occupation).Avoid patient identifiers (date of birth, initials).Describe the patient's complaint.List the patient's present illness.List the patient's medical history.More items...•
How do you make a report?
How to write a report in 7 steps1 Choose a topic based on the assignment. Before you start writing, you need to pick the topic of your report. ... 2 Conduct research. ... 3 Write a thesis statement. ... 4 Prepare an outline. ... 5 Write a rough draft. ... 6 Revise and edit your report. ... 7 Proofread and check for mistakes.
What are the types of reports in nursing?
There are different types of nursing reports described in the literature, but the four main types are: a written report, a tape-recorded report, a verbal face-to-face report conducted in a private setting, and face-to-face bedside handoff.
How do you end a shift report?
5 Tips for an Effective End-of-Shift ReportGive a Bedside Report. “Check pertinent things together such as skin, neuro, pulses, etc. ... Be Specific, Concise and Clear. “Stay on point with the 'need to know' information. ... When in Doubt, Ask for Clarification. ... Record Everything. ... Be Positive!
What is SBAR template?
SBAR is an acronym for Situation, Background, Assessment, Recommendation. It is a technique used to facilitate appropriate and prompt communication. An SBAR template will provide you and other clinicians with an unambiguous and specific way to communicate vital information to other medical professionals.
How do nurses give good reports?
1:1611:43How to Give a Good Nursing Shift Report (with nursing report sheet ...YouTubeStart of suggested clipEnd of suggested clipAll. Right guys here we are looking at our handoff. Report and assessment sheet this is the sheetMoreAll. Right guys here we are looking at our handoff. Report and assessment sheet this is the sheet that I recommend that you print out about 30 minutes before the end of any shift and print out one for
Does Etsy offer free shipping?
Shipping policies vary, but many of our sellers offer free shipping when you purchase from them. Typically, orders of $35 USD or more (within the s...
How do I personalize items on Etsy?
Found something you love but want to make it even more uniquely you? Good news! Many sellers on Etsy offer personalized, made-to-order items. To pe...
Does shopping on Etsy help support small businesses?
Absolutely! Our global marketplace is a vibrant community of real people connecting over special goods. With powerful tools and services, along wit...
How to have a smooth shift change?
Reporting is the best way to have a smooth nursing shift change. Oral communication may not always help. One or two emergency cases can be reported orally to the oncoming nurse for providing immediate care. However, not all can be remembered. It is a good practice to use shift change sheet as an effective communication tool in between nurse.
What is shift change report?
Therefore the communication between nurses about the patient is recorded and is called as a shift change report.
What time does a nurse leave a hospital?
This time varies from hospital to hospital it can be from 3 AM to 3 PM, 9 AM to 9 PM etc. However, there is a shift and of course, the nurse will leave hospital handing over the responsibility to the duty nurse. Unlike another profession, nursing job deals with people who are sick.
What is the duty of a nurse?
During duty, the nurse will attend many patients. Each one will have a different history, diagnosis, allergies to medicine, medicine, food etc. It is vital that the nurse make a note of that and pass on to the other nurse who takes duty. Whether or not medicine is given and other details to be informed to the doctor or patients relatives are noted down in the shift change report.
What is the patient identification heading?
Under the patient identification heading the patient’s name, id number given in the hospital, room number, age, gender, date of birth must be mentioned. Additional details like a patient’s father or spouse name and contact details also can be given in case if any emergency call needs to be placed by the nurse.
Do nurses feel panicked about ICU duty?
We understand that nurses feel panic about attending ICU duty. Patients in the intensive care unit need extra attention and hence nurses must be vigilant all the time. So let us see how they can use the change report sheet for their best use.
Can an ortho patient have one doctor?
For instance, a patient with an ortho problem will have one doctor who will treat. Others may be checking the patient for different reasons like surgery recommendation etc. But the primary doctor details to be presented for the nurse to reach out for any help at critical condition.
You Need a Nursing Brain Sheet That Works for YOU
For the longest time I have tried pushing the brain sheet that worked for me onto new students and newbie nurses. I’ve changed my tone.
The Nursing Brain Sheet Database
The response was AMAZING (to say the least). We received over 100 report sheet templates from nurses working in MedSurg, ICU, ED, OB, Peds, Tele . . . you name it.
1. Handoff and Nursing Report Sheet
This is the report sheet that my preceptor used to make me fill out prior to the end of each shift as a newbie. To be honest, at first I was so annoyed that I had to spend like an hour at the end of each shift filling this out. It wasn’t until I realized I was able to give a badass report that I was finally grateful she made me fill this out.
3. 4 Patient Simple Tele Sheet
Some people like it simple . . .this is the sheet for you. With slight prompting this sheet makes a great tool for the MedSurg or Tele nurse on the GO!
4. 4 Patient Simple Nurse Task Sheet
I love this one. At first glance it looks basic . . . put at closer inspection you start to see all the details and information you have available with it. From lab values, to foley care, to last pain med, this is would be a great one for a nurse that has a flow and just wants a simple push to stay a bit more organized.
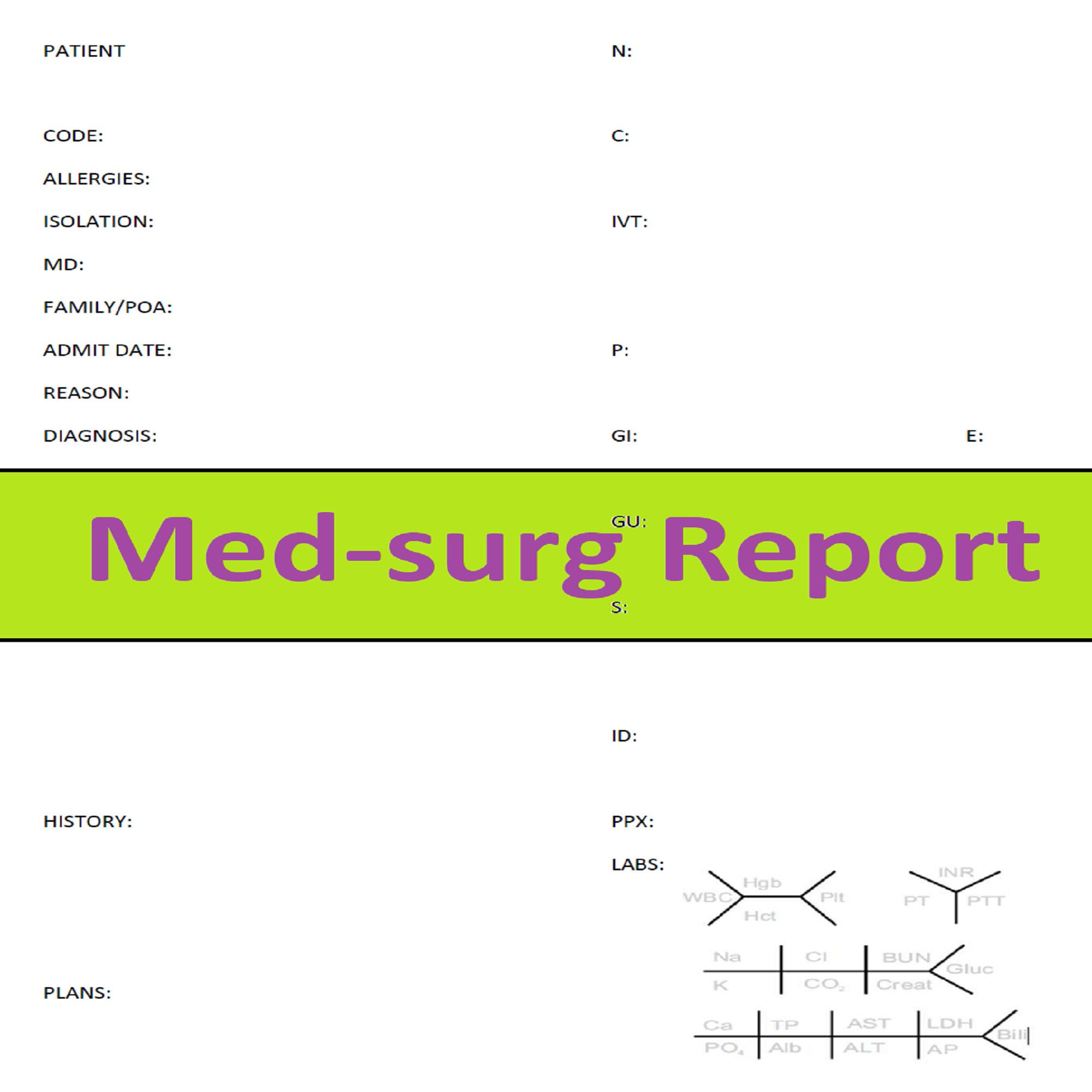
5. Vertical Nurse Brain sheet with Assessment Diagram
I’m a visual learner. This one just grabs my attention. I like the top section for the “essentials” like blood sugars, DX, and Pt info. I also really like the area below the charts to draw little notes about your physical assessment. I really like this nursing brain sheet for beginner or experience nurse.
6. Just the Boxes
I’ll be honest . . . after a couple years of being a nurse my “brainsheet” has evolved into more of a few freehand drawing on a sheet of paper. If that sounds like you, this is probably the one for you. With little more than a few suggestions . . . this is a pretty basic organizer for nurses.
What is an organization sheet in med sg?
What a Med Surg organization sheet contains? At the Med Surg department, there are certainly organization sheets that are part of their duties. Contains data about patients in the scope of their care. For example, the room where the patient was treated, the name of the patient, the contact of the person closest to the patient, ...
What is a med sage?
Med Surg stands for medical-surgical which is a department that contains nurses specifically handling patients who need recovery after undergoing surgery. There is no specific age for patients treated by Med Surg nurses. To be sure, after undergoing surgery, patients will find it difficult to move the body and there are even some patients who need ...
Why is the knowledge possessed by each nurse so different?
The knowledge possessed by each nurse is very different because, in their studies, they have focused on one department. So that the action that can be taken by all the nurses initially is general medical knowledge.