Portal Vein: Anatomy, Function, and Significance
7 hours ago · The portal vein (PV) is the main vessel of the portal venous system (PVS), which drains the blood from the gastrointestinal tract, gallbladder, pancreas, and spleen to the liver. There are several variants affecting the PV, and quite a number of congenital and acquired … >> Go To The Portal
Which veins drain directly into the portal vein?
Notable characteristics of chronic liver disease can include:
- ascites
- esophageal varices
- spider nevi
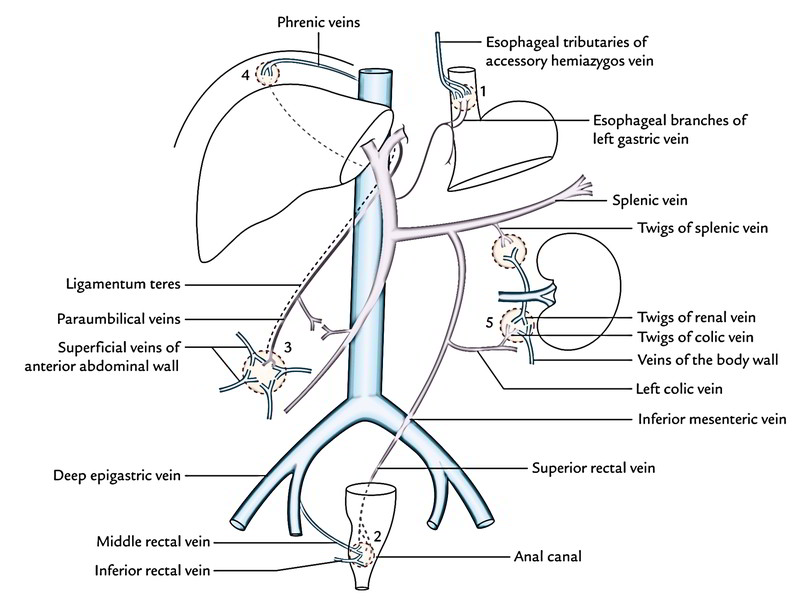
- caput medusae
- palmar erythema
What is a prominent portal vein?
- Evaluation of your medical history
- A physical exam
- Blood tests
- Angiogram (an X-ray test that takes pictures of the blood flow within a particular artery)
- Ultrasound
- Endoscopy
What is the normal size of portal vein?
What Does Liver Size Say About My Health?
- Normal liver size by age. Men tend to have a larger liver size than women. This is usually because men’s bodies tend to be larger.
- Causes of an enlarged liver. The condition of having an enlarged liver is called hepatomegaly. ...
- Practicing good liver health. Maintain a healthy weight for you. ...
- Takeaway. The liver is an important organ that grows as you age. ...
What is the normal flow of the portal vein?
Normal portal venous flow should be continuous with slight respiratory variation. Normal venous flow should be more pulsatile with a “tango sign” of 2 steps forward 1 step back. That is flow toward the IVC then reversed flow with the atrial contraction.
See more

What is the main portal vein?
The portal vein (PV) is the main vessel of the portal venous system (PVS), which drains the blood from the gastrointestinal tract, gallbladder, pancreas, and spleen to the liver. There are several variants affecting the PV, and quite a number of congenital and acquired pathologies.
What happens when portal vein is blocked?
Portal vein thrombosis is blockage or narrowing of the portal vein (the blood vessel that brings blood to the liver from the intestines) by a blood clot. Most people have no symptoms, but in some people, fluid accumulates in the abdomen, the spleen enlarges, and/or severe bleeding occurs in the esophagus.
When do you treat Pvt?
For both patients with acute and patients with chronic PVT, treatment is recommended for at least 3 months, with an indefinite duration for patients with permanent risk factors or with extension to the mesenteric veins. Indefinite duration treatment is recommended for all patients with BCS.
What are the four major clinical manifestation of portal hypertension?
The clinical manifestations of portal hypertension may include caput medusae, splenomegaly, edema of the legs, and gynecomastia (less commonly) (Figure 2). Caput medusae is a network of dilated veins surrounding the umbilicus.
How long can you live with portal vein thrombosis?
In adults with portal vein thrombosis, the 10-year survival rate has been reported to be 38-60%, with most of the deaths occurring secondary to the underlying disease (eg, cirrhosis, malignancy).
What is the most common complication of portal hypertension?
Variceal hemorrhage is the most common complication associated with portal hypertension. Almost 90% of patients with cirrhosis develop varices, and approximately 30% of varices bleed.
Can Pvt be cured?
Portal vein thrombosis is a serious condition. If caught early, PVT can be treatable with noninvasive procedures and treatment.
How can I stop Pvt?
In a single randomised trial, anticoagulation with low-molecular-weight heparin (LMWH) in patients with advanced cirrhosis was efficacious in preventing PVT and reducing the risk of worsening decompensation.
What are the symptoms of PVT?
Acute PVT may be marked by abdominal pain, nausea, and/or vomiting, low back pain, and fever in the setting of septic portal vein thrombus (pylephlebitis). While a systemic inflammatory response may be seen in PVT, if there is evidence of high fever, chills, and bacteremia, pylephlebitis may be present.
What is the most common cause of portal hypertension?
Portal hypertension is elevated pressure in your portal venous system. The portal vein is a major vein that leads to the liver. The most common cause of portal hypertension is cirrhosis (scarring) of the liver.
What are the three categories of portal hypertension?
With regard to the liver itself, causes of portal hypertension usually are classified as prehepatic, intrahepatic, and posthepatic.
Is portal hypertension serious?
Portal hypertension is a dangerous condition with severe, life-threatening complications. Call your healthcare provider right away if you notice any of these symptoms: Yellowing of the skin. Abnormally swollen belly.
What is the main vessel of the portal vein?
The portal vein (PV) is the main vessel of the portal venous system (PVS), which drains the blood from the gastrointestinal tract, gallbladder, pancreas, and spleen to the liver. There are several variants affecting the PV, and quite a number of congenital and acquired pathologies.
What percentage of people have portal veins?
The typical branching pattern of the main portal vein occurs in 65% of individuals in the general population.
What is a portosystemic shunt?
Portosystemic shunts are diversions of portal venous blood into the systemic venous system bypassing the liver. Patients may be asymptomatic, but high-flow shunts are prone to develop hepatic encephalopathy, hepatopulmonary syndrome, and portopulmonary syndrome. Depending on the case, these shunts are managed conservatively, with trans-catheter embolization, or surgery.
What is the best imaging technique for PVS?
In most centers, CT is the preferred technique for the evaluation of the PVS, permitting the evaluation of the portal vasculature using high-resolution isotropic acquisition in a short time, and allowing high-quality multiplanar reformations (MPR) and three-dimensional reconstructions [3]. In addition, multiphasic CT allows a comprehensive evaluation of the entire porta hepatiswith high temporal and spatial resolution. MRI can also be used to evaluate the PVS. The major advantage is the possibility to anatomically evaluate and obtain information about the contents of vascular structures without administering intravenous contrast product and non-using ionizing radiation. However, compared to CT, it is still a more time-consuming, expensive, and less accessible imaging technique, generally with less spatial and temporal resolution necessary to evaluate vascular structures, and also more susceptible to artifacts. Doppler ultrasound is a useful imaging technique in the evaluation of the PVS, is highly available, and the major advantage is allowing a detailed evaluation of the venous flow besides the anatomical information. Sometimes it is conditioned by the biotype and lack of collaboration of the patient, and still have to recur to other techniques if necessary an overall PVS assessment or dynamic contrast information.
What are the two paired veins in the PV?
aThe vitelline venous system arrives at the primitive liver as two paired veins (right and left), branches into the hepatic sinusoids, and then coalesce, pierce the septum tranversum(primitive diaphragm) and drain into the sinus venosus(primitive heart). These two vitelline veins communicate through three pre-hepatic anastomoses around the developing duodenum (cranial-ventral, dorsal, and caudal-ventral). bOver time, a selective involution occurs, involving the caudal part of the right vitelline vein, the cranial part of the left vitelline vein, and the caudal-ventral anastomosis. The dorsal and cranial-ventral anastomoses persist and give rise to the main PV and to the left PV, respectively. Initially, the paired umbilical veins lie more lateral than the vitelline ones, and also pierce the septum tranversumand drain into the sinus venosus. With the development of the liver, the umbilical veins fragment and connect to the hepatic sinusoids. Over time, a selective involution of the right umbilical vein and cranial portion of the left umbilical vein also occurs. cThe remnant left umbilical vein cranially bifurcates, forming two new communications: one with the IVC through the ductus venosus, carrying oxygenated blood from the placenta directly to the fetus; and another with the left PV, supplying directly the liver. After birth, the ductus venosusand the left umbilical vein involute and become the ligamentum venosumand ligamentum teres, respectively
What is the main vessel of the PVS?
The portal vein (PV) is the main vessel of the PVS, resulting from the confluence of the splenic and superior mesenteric veins, and drains directly into the liver, contributing to approximately 75% of its blood flow [1]. Hepatic artery provides the remaining hepatic blood flow. Once in the liver, PV ramifies and reaches the sinusoids, with downstream blood being directed to the central vein at the hepatic lobule level, then to the hepatic veins and inferior vena cava (IVC) to reach the systemic venous system.
What is the splenic vein?
On normal anatomy, typically, the splenic vein (SV) joins the superior mesenteric vein (SMV) anteriorly to the IVC and posteriorly to the pan creatic neck to form the PV, which ascends within the hepatoduodenal ligament, posteriorly to the hepatic artery and common bile duct, toward the hepatic hilum, where it divides into right and left (Fig. 2a). The left PV is horizontal for a short distance before it turns cranially and branches, supplying Couinaud hepatic segments I, II, III, and IV. The right PV subdivides into anterior and posterior branches; the anterior one supplying segments V and VIII, and the posterior branch supplying segments VI and VII. This typical branching pattern of the main PV occurs in 65% of individuals in the general population [2] (Fig. 2b). Additional tributaries of the PV include the left and right gastric veins, cystic veins, and Sappey veins. The inferior mesenteric vein (IMV) has greater variability, joining the splenic vein (40%), the SMV (40%), or the splenomesenteric confluence (20%) [2].
How does a portal vein thrombosis drug work?
This drug helps to reduce blood flow to the liver and reduces pressure in the abdomen. In order to stop bleeding, this medication may be injected directly into the veins. If you develop portal vein thrombosis from an infection — specifically for infants — doctors may prescribe antibiotic medication to cure the source.
What is the best imaging for portal vein thrombosis?
Doppler ultrasounds, on the other hand, can use imaging to display blood circulation within the vessels. This can be used to diagnose your portal vein thrombosis and determine how severe it is. 2. CT Scans.
What is a PVT?
Portal vein thrombosis (PVT) is a blood clot of the portal vein, also known as the hepatic portal vein. This vein allows blood to flow from the intestines to the liver. A PVT blocks this blood flow. Although PVT is treatable, it can be life-threatening.
How to stop bleeding from varicose veins?
To stop the bleeding, rubber bands are inserted through the mouth into the esophagus to tie off the varicose veins.
Why do blood clots form?
Blood clots are more likely to form when the blood flows irregularly in the body. While doctors typically don’t know what causes portal vein thrombosis, there are a number of risk factors for developing this condition. Some of the most common include:
What to take if you have a PVT?
If you have a more severe case of PVT that is causing your esophagus to bleed, your doctors may also recommend taking beta-blockers. These help reduce pressure in the portal vein and stop the risk for any excess bleeding.
What is the best treatment for PVT?
For acute PVT, doctors commonly recommend medication as thrombolytic treatment . These prescription drugs can dissolve blood clots. For gradual clot growth, patients may be prescribed anticoagulant drugs — blood thinners such as heparin — to help prevent recurrent clots and any excess growth.
What is the main vessel in the portal vein?
Portal vein. The portal vein (PV) (sometimes referred to as the main or hepatic portal vein) is the main vessel in the portal venous system and drains blood from the gastrointestinal tract and spleen to the liver.
How big is a portal vein?
The portal vein usually measures approximately 8 cm in length in adults with a maximum diameter of 13 mm. It originates posterior to the neck of the pancreas where it is classically formed by the union of the superior mesenteric and splenic veins (the portovenous confluence).
What is the portal system?
A portal venous system is one in which veins connect two capillary beds; or in other words drain one organ/organ system and pass into another organ/organ system rather than being directly returned to the heart. The hepatic portal vein is the only portal system many are aware of. However, there is also a hypophyseal portal system which passes blood from the hypothalamus to the anterior pituitary 8.
What is the incidence of portal vein variation?
The overall incidence of portal vein variation is reported to be ~25% (range 20-30%), which should be recognized prior to procedures such as liver transplantation, complex hepatectomy and portal vein embolization 2-4 :
Where does the left portal vein originate?
The main branches of the left portal vein originate from the umbilical portion , and supply liver segments 2, 3 and 4 5. The portal vein ramifies further, forming smaller venous branches and ultimately portal venules.
Where does the blood supply to the liver come from?
These vessels ultimately empty into the hepatic sinusoids to supply blood to the liver. 75% of the blood supplied to the liver comes from the portal vein, but it only supplies 50% of the oxygen supply to the liver.
Where do the embryonic vitelline veins drain from?
The embryonic vitelline veins drain from the yolk sac to the sinus venosus. The two vitelline veins develop anastomosing cross-communications around the duodenum, in the developing liver and the septum transversum. Selective involution of these veins leads to the formation of the portal vein and rotation of the foregut contributes to the formation of its extra-hepatic course 6.
What is portal vein thrombosis?
Portal vein thrombosis (PVT) refers to thrombosis that develops in the trunk of the portal vein including its right and left intrahepatic branches and may even extend to the splenic or superior mesenteric veins or towards the liver involving intrahepatic portal branches. PVT occurs either in association with cirrhosis or malignancy of liver or may occur without an associated liver disease. The terminology of Extra Hepatic Portal Venous Obstruction (EHPVO) refers to the development of portal cavernoma in the absence of associated liver disease. EHPVO should be considered as a separate entity. Portal vein thrombosis is an important cause of non-cirrhotic prehepatic portal hypertension all over the world.
What is the sensitivity of a portal vein ultrasound?
Ultrasound is the investigation of choice. It shows solid isoechoic or hypoechoic material within portal vein either filling the lumen partially or complete.88It is the least expensive method but sensitivity and specificity is affected by interpatient variability and expertise of the given radiologist.89Overall the sensitivity and specificity of ultrasound for detecting portal vein thrombosis ranges from 80 to 100% with an accuracy of 88–98%. Demonstration of a portal cavernoma (multiple tortuous small vessels replacing the portal vein) is suggestive of chronic PVT, and is usually associated with splenomegaly and collaterals in relation to portal venous system. Color Doppler ultrasonography (CDUS) and Pulsed Wave ultrasonography (PWUS) demonstrated the absence or reduced flow in portal vein. The diagnostic sensitivity and specificity for Color Doppler Ultrasound (CDUS) in detecting portal vein thrombosis varies from 66% to 100%.90,91Contrast enhanced ultrasound (CDUS) is another modality that has been found to be superior to ultrasound in demonstrating the presence or absence of flow and is more reliable in patients with extremely low portal vein velocity. Endoscopic ultrasound has also been reported to be a sensitive (81%) and specific (93%) test to diagnose portal vein thrombosis.92–94Gallbladder varices on ultrasound have been seen in 12–30% of adults with chronic PVT.95
What is the mortality rate for portal vein thrombosis?
Mortality in the past was 20%–50% with acute portal vein thrombosis and other splanchnic vessels, but with an early diagnosis, increased clinical awareness, improved diagnostic techniques and use of early anticoagulation the 5 yr survival rate has improved to 85%.110,111Outcome of PVT is generally good and mortality primarily is due to underlying cause and less to consequences of portal hypertension. Acute PVT usually has a good prognosis when treated before the occurrence of intestinal infarction. However in the event of bowel infarction and multi organ failure, the in hospital mortality is approximately 20–50%.112Mortality is highest at one year in patients with cancer or cirrhosis compared with those without (26% vs 8%).40Bleeding related mortality in patients with PVT is much lower than in patients with cirrhosis due to preserved liver function.
How does portal hemodynamics affect cirrhosis?
In cirrhosis, portal hemodynamics play an important role in the development of portal vein thrombosis. A study by Zocco et al showed portal flow velocity of less than 15 cm/s on Doppler ultrasound as a predictive factor for the development of portal vein thrombosis with a risk of 47.8% when compared to 2% risk with a flow of more than 15 cm/s.63The parenchymal architectural distortion in cirrhosis and altered vascular reactivity results in increased intrahepatic vascular resistance and reduction in portal blood flow. The development of portosystemic collateral circulation and splanchnic vasodilatation on venous side also adds to stagnation of the portal blood flow leading to PVT. A recent study has also shown that in patients with PVT, the largest collateral vessel blood flow was an independent predictor of PVT. The blood flow velocity in the largest collateral (>10 cm/s) and flow volume (>400 ml/min) were associated with increased incidence of portal vein thrombosis in virus related cirrhosis.64
What is PVT in liver?
PVT occurs either in association with cirrhosis or malignancy of liver or may occur without an associated liver disease. The terminology of Extra Hepatic Portal Venous Obstruction (EHPVO) refers to the development of portal cavernoma in the absence of associated liver disease.
When was PVT first described?
Balfour and Stewart described the first case of PVT in 1868 in a patient with ascites, splenomegaly and variceal dilation.1Since then portal vein thrombosis has been well studied and described in patients with or without cirrhosis.
How to differentiate acute from chronic PVT?
An easy way to differentiate acute PVT from chronic PVT is the absence or insignificant portoportal collaterals on imaging and no evidence of portal hypertension including splenomegaly and esophageal varices. The proportion of patients who develop chronic PVT from acute is known for those who develop symptomatic PVT recognized early however it is unclear for those who develop asymptomatic PVT.
What is the hepatopetal flow in the main portal vein?
What is Hepatopetal flow in the main portal vein? Hepatopetal denotes flow of blood towards the liver, which is the normal direction of blood flow through the portal vein. The term is typically used when discussing the portal vein or recanalized vein of the ligamentum teres in patients with suspected portal hypertension.
What is the peak velocity of a portal vein?
Sluggish or Slow Portal Venous Flow Normal main portal vein (MPV) peak systolic velocities range between 20 cm/sec and 40 cm/sec. A low flow velocity of <16 cm/sec in addition to a caliber increase in the MPV are diagnostic features of portal hypertension [7].
What is the blood vessel that carries blood from the gastrointestinal tract, gallbladder, pancreas?
The portal vein or hepatic portal vein is a blood vessel that carries blood from the gastrointestinal tract, gallbladder, pancreas and spleen to the liver. This blood contains nutrients and toxins extracted from digested contents. The blood leaves the liver to the heart in the hepatic veins.
What happens during portal circulation?
Secondly, what occurs during portal circulation? In the circulatory system of animals, a portal venous system occurs when a capillary bed pools into another capillary bed through veins, without first going through the heart. For this reason, portal vein most commonly refers to the hepatic portal vein.
Why do people with cirrhosis have portal vein thrombosis?
Causes. About 25% of adults with cirrhosis have portal vein thrombosis, usually because blood flow through the severely scarred liver is slow. When blood flow is slow, blood is more likely to clot. Any condition that makes blood more likely to clot can cause portal vein thrombosis.
What is the liver doppler?
The Liver Doppler Ultra sound assesses the blood that flows into the liver through the portal veins and the blood that flows out of the liver through the hepatic veins which empty into the heart. Liver Doppler is also used to evaluate the liver on a regular basis in people who have had a liver transplant.
What causes high blood pressure in the liver?
It occurs when cells in your liver become damaged and your body can't repair them. Your body carries blood to your liver through a large blood vessel called the portal vein. Cirrhosis slows your blood flow and puts stress on the portal vein. This causes high blood pressure known as portal hypertension.
Can a splenic vein develop in tandem with a portal vein?
Isolated splenic vein thrombosis can develop in tandem with a patent portal vein. However, it is unusual to have thrombosis of the inferior/superior mesenteric veins without involvement of the portal vein itself. Finally, there is the possibility of mesenteric venous thrombosis, where every vessel in the abdomen is thrombosed.
Can you use anticoagulant for nonbleeding varices?
Most patients fall between these two extremes. Patients with nonbleeding varices and PVT should be anticoagulated in the hope of recanalization of the portal vein. If the patient is imaged and a partial thrombosis of the portal vein is found, I would anticoagulate to avoid completion of the process and the onset of symptoms. In extremely rare cases, these patients, if left untreated, could develop bowel ischemia and, ultimately, a bowel infarction. If anticoagulant therapy is prescribed in stable, asymptomatic patients, heparin is not necessary. If the PVT is found incidentally, patients can be maintained on warfarin, especially if a prothrombotic disorder is present.
Can a PVT be used in place of a portal vein?
At the time of transplant, PVT is also a potential issue in cirrhotics because the portal vein cannot be connected to the new liver. If the transplant patient has a patent inferior mesenteric vein, it can be used in place of the portal vein, but if the entire portal venous system is thrombosed, transplant is not an option. Fortunately, in cirrhotic patients, thrombosis of the mesenteric vascular system is very uncommon.
What does it mean to say portal and hepatic veins are patent?
Evaluation liver: Portal vein is the main blood flow to the liver it occluded sometime with thrombosis that is usually treated with blood thinners like Coumadin ( warfarin) . Hepatic veins drains blood from liver to the heart , if they occlude the patient will develop jaundice and sometimes severe liver dysfunction .
What do you mean by hepatic veins and portal veins are patent?
Patent = open: It sounds like you've gotten a report from an imaging study, such as CT, MRI, or ultrasound (or even certain types of surgery or procedure).
Terminology
- The portal vein is formed by the confluence of the splenic vein, which brings blood from the spleen, and the superior mesenteric vein, which brings blood from the intestines. Smaller veins from the stomach and pancreas also contribute to portal vein blood flow. The splenic vein and superior mesenteric vein join behind the neck of the pancreas to fo...
Gross Anatomy
Relations
Variant Anatomy
Development
- The portal vein usually measures approximately 8 cm in length in adults with a maximum diameter of 13 mm.9 It originates posterior to the neck of the pancreas where it is classically formed by the union of the superior mesenteric and splenic veins (the portovenous/portomesenteric confluence). 3 The origin of the vein defines the location of the pa…
Related Pathology
- anterior - the neck and body of the pancreas, D1 segment of duodenum
- posterior - inferior vena cava