10+ Patient Care Report Examples [ EMS, EMT, …
3 hours ago A patient care report is a document written by medical professionals to report about the patient’s wellbeing, care and status. This document consists of the result of the assessment and the evaluation of the patient being done by the EMTs or the EMS. >> Go To The Portal
How do you write a patient assessment?
Assessment & PlanWrite an effective problem statement.Write out a detailed list of problems. From history, physical exam, vitals, labs, radiology, any studies or procedures done, microbiology write out a list of problems or impressions.Combine problems.
What is included in a patient assessment?
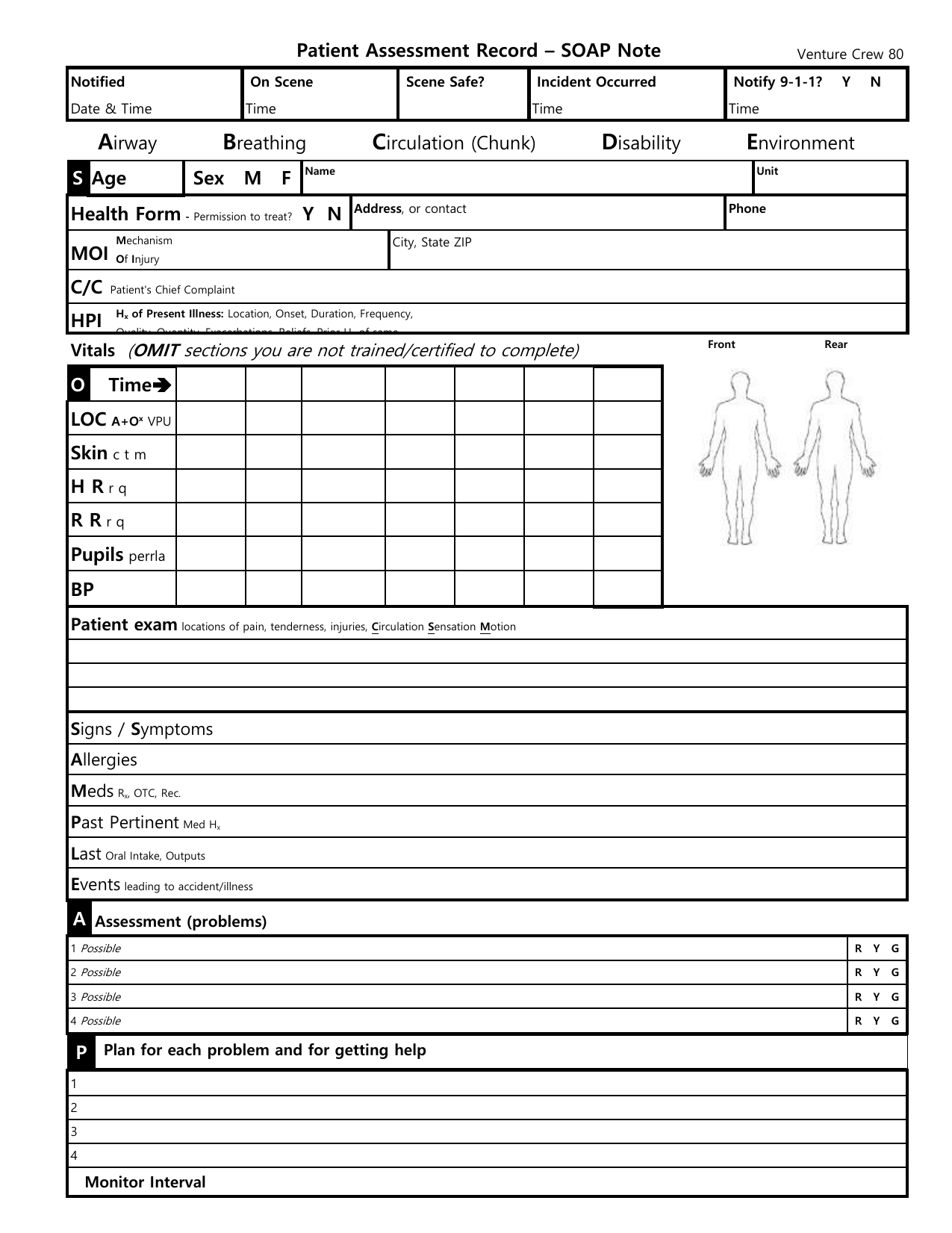
A comprehensive health assessment gives nurses insight into a patient's physical status through observation, the measurement of vital signs and self-reported symptoms. It includes a medical history, a general survey and a complete physical examination.
What is an example of assessment in nursing?
For example, a nurse's assessment of a hospitalized patient in pain includes not only the physical causes and manifestations of pain, but the patient's response—an inability to get out of bed, refusal to eat, withdrawal from family members, anger directed at hospital staff, fear, or request for more pain mediation.
What are the five components of patient assessment?
emergency call; determining scene safety, taking BSI precautions, noting the mechanism of injury or patient's nature of illness, determining the number of patients, and deciding what, if any additional resources are needed including Advanced Life Support.
What is patient assessment in nursing?
Patient assessment is the foundation of any plan of care. This zone collates essential clinical content to help nurses refresh their knowledge of the underlying principles of assessment and the skills required to help plan and evaluate patient care.
What is a detailed assessment of a patient's medical history?
Medical charts contain documentation regarding a patient's active and past medical history, including immunizations, medical conditions, acute and chronic diseases, testing results, treatments, and more.
How do you write a nursing assessment summary?
The following are comprehensive steps to write a nursing assessment report.Collect Information. ... Focused assessment. ... Analyze the patient's information. ... Comment on your sources of information. ... Decide on the patient issues.
What are the 5 types of nursing assessments?
Nurses can perform focused assessments in any of these areas:Neurological assessment.Respiratory assessment.Cardiovascular assessment.Gastrointestinal assessment.Renal assessment.Musculoskeletal assessment.Skin assessment.Eye assessment.More items...•
What are the 4 types of nursing assessment?
4 types of nursing assessments:Initial assessment. Also called a triage, the initial assessment's purpose is to determine the origin and nature of the problem and to use that information to prepare for the next assessment stages. ... Focused assessment. ... Time-lapsed assessment. ... Emergency assessment.
What are the 8 general principles for patient assessment?
Overview of Picker's Eight Principles of Patient Centered CareRespect for patients' values, preferences and expressed needs. ... Coordination and integration of care. ... Information and education. ... Physical comfort. ... Emotional support and alleviation of fear and anxiety. ... Involvement of family and friends. ... Continuity and transition.More items...•
What is the very first step in your patient assessment?
Patient assessment starts before you arrive at the patient's side with a scene size-up. The first step is always to assess the possible risks and take appropriate precautions. The importance of assessing scene safety cannot be overestimated.
What is the final step of patient assessment?
Evaluation phase The final phase of the nursing process is the evaluation phase. It takes place following the interventions to see if the goals have been met. During the evaluation phase, the nurse will determine how to measure the success of the goals and interventions.
What are the 8 general principles for patient assessment?
Overview of Picker's Eight Principles of Patient Centered CareRespect for patients' values, preferences and expressed needs. ... Coordination and integration of care. ... Information and education. ... Physical comfort. ... Emotional support and alleviation of fear and anxiety. ... Involvement of family and friends. ... Continuity and transition.More items...•
How do you take general assessment of a patient?
Patient assessment commences with assessing the general appearance of the patient. Use observation to identify the general appearance of the patient which includes level of interaction, looks well or unwell, pale or flushed, lethargic or active, agitated or calm, compliant or combative, posture and movement.
What would be considered an objective patient assessment finding?
Examples of objective assessment include observing a client's gait , physically feeling a lump on client's leg, listening to a client's heart, tapping on the body to elicit sounds, as well as collecting or reviewing laboratory and diagnostic tests such as blood tests, urine tests, X-ray etc.
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the inf...
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very caref...
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make...
What is a new patient assessment form?
A new patient assessment form is a type of assessment form that is used as a means of assessing and grading a person development before and after they have entered the medical institution. This is typically done as a means of determining the state of health a patient was in prior to their admission to the hospital.
What is the purpose of filling out a patient assessment form?
Filling out a patient assessment form will require you to understand the current medical condition of the patient so as to understand and determine what their standard of health. Here is a guide on how to fill out a patient assessment form:
What is a health assessment?
This is done like clockwork to monitor a patient’s recovery, as well as the development of whatever ailment they may have at the time.
Why do hospitals do self assessment?
This is often done to ensure that the hospital’s patients are recovering at a steady pace. However, patients are often encouraged to undergo a self-assessment using a self-assessment form to help the patient develop their psychological recovery as well.
How to describe a patient?
Begin by identifying your patient, give a full description like height, weight, name, age, gender, date of birth, blood type, allergies, medical ailments, skin tone and etc.
Is it easy to write a patient assessment report?
Writing a patient’s assessment report can be easy or difficult depending on your experience making the reports it will also depend on how thorough and how well you made your patient assessment formprior to the creation of this patient assessment report, Now, to begin making a patient assessment report you need to:
Why are patient reports important?
Why Patient Reports Are Needed. Patient medical reports serve as evidences that the patient has been given proper medications or treatments. Doctors or physicians are doing the best they could in order to supply the needs of each and every patient, regardless if they are in a critical condition or not.
Why do we need a patient report?
These patient reports also help the doctors and the relatives of the patient to know what is or are behind the patients’ results of their individual health assessment . Thus, the form for patient report contains all the fields for information and exact details that are needed to be provided. In other words, the patient report forms are organized and layered which makes it easier to be filled with all the relevant information. And when all the precise information are provided, it is much easier to assess or evaluate the current state of one’s health condition.
Why is a patient's medical record required?
Patient medical reportsserve as evidences that the patient has been given proper medications or treatments. Doctors or physicians are doing the best they could in order to supply the needs of each and every patient, regardless if they are in a critical condition or not. These reports are mandatory for the individual patient. This is for the reason that these are part of their health or medical history. Therefore, it is mandatory that the medical clinic, center, or hospital keeps a record of their patients.
What is the relevant information needed for a patient complaint?
In a patient complaint, the relevant information that are needed are as follows: The description of the situation. The effect on privacy.
What is healthcare personnel?
Healthcare personnel in hospitals or medical centers ensure that they provide the needs of the patients (pertaining to the treatments or medications needed) and their individual relatives (pertaining to the answers or provision of exact details from the medical results). It goes without saying that everyone wants an accurate general information ...
Can medical records be shared with other people?
Yet, these medical reportsor records should not be shown to other unauthorized people. The reason for this is because these files are confidential, and the only people who could have access to these are those who are authorized, unless the patient or the owner of the records gives his or her consent for the informationto be released to certain people or to the public. Otherwise, the clinic, center, or hospital are held accountable for such infringement with regards to the confidential information.
Do hospitals keep records of patients?
Therefore, it is mandatory that the medical clinic, center, or hospital keeps a record of their patients. These patient reports also help the doctors and the relatives of the patient to know what is or are behind the patients’ results of their individual health assessment.
What is assessment section?
The assessment section is where you document your thoughts on the salient issues and the diagnosis (or differential diagnosis), which will be based on the information collected in the previous two sections.
When to use quotation marks in a patient response?
You should document the patient’s responses accurately and use quotation marks if you are directly quoting something the patient has said.
How many OSCE checklists are there?
If you'd like to support us and get something great in return, check out our OSCE Checklist Booklet containing over 150 OSCE checklists in PDF format. You might also be interested in our Clinical Skills App and our OSCE Flashcard Collection which contains over 2000 cards.
What should be included in subjective documentation?
The subjective section of your documentation should include how the patient is currently feeling and how they’ve been since the last review in their own words.
What is the final section of a review?
The final section is the plan, which is where you document how you are going to address or further investigate any issues raised during the review.
Do you need to tell us which article this feedback relates to?
You don't need to tell us which article this feedback relates to, as we automatically capture that information for you .
Can you comment on a diagnosis that is already known?
If the diagnosis is already known and the findings of your assessment remain in keeping with that diagnosis, you can comment on whether the patient is clinically improving or deteriorating:
What is a Psychological Assessment Report?
A psychological assessment report is a document that contains the psychological assessment of a person. Psychological assessment is the way of testing the behaviour, personality and abilities of a person using techniques where the psychologist can arrive with hypotheses. It can also be called psychological testing. The assessment states whether a person is suffering from a mental illness or not. The purpose of this report is to give information about the mental conditions of a person. It is used in a variety of ways. Companies commonly used psychological testing as a part of recruitment process in hiring. Psychological report is used in children to assess whether they are normal or not. It can also be used in court as an evidence that can help in the trial. Not that mental health should be in question, but the fact that we know the mental condition of a person can help the person who can have the illness and the people around us. We have to be a little concerned about our mental health. We have to know the mental history of an individual. We can help them if we will do so. If an employee was proved to have a mental illness, we can be careful about his condition while we are at work. In case of our children, bringing them to the psychologist at an early age can make us to give an early solution if there could ever be found a diagnosis of mental problem. The psychological assessment report is useful and we can take care of our mental health.
Why is it important to write a psychological report?
Writing a psychological report is crucial as it would contain the delicate issue about the mental health of a person. If you are new in psychological assessment report writing, you might want to try these steps in writing:
How Can I Make My Psychological Report Writing Better?
Be sure that you are going to include accurate information only. To have some great skills, use any psychological assessment example as a reference. You can have better ideas on how to write a psychological report.
How to interview a patient?
As you do the interview with the patient, you must do it with proper care. Speak in a warm tone and ask questions that will not hurt the feelings of the patient. You have to remember, be a good counselor to your patient. To get the best counsel, do not make the interview short. Take a great time to let the patient speak their thoughts, so you can know if they have a problem or not. Apply all the knowledge that you have learned in your psychology course. You may have learned some great skills on how to handle a patient. Do not ask too personal questions instantly. Let the patient open that kind of conversation. Remember that our thoughts are too personal to be intruded. Before a patient would hide themselves because of awkwardness, ask questions that would make them feel more at ease with you. They might open up if you will choose right questions. One of the best way is to ask how they are doing. Ask what is going on with their thoughts. Ask if something has been troubling them. Ask all of these in a friendly tone where anyone can tell their worries and fear.
Why Should We Have To Undergo a Psychological Assessment?
There are various reasons why we have to undergo a psychological assessment. Sometimes we have difficulties and we have to take the psychological testing to assess the problem that we are having. We can know if we are struggling with a mental problem. We can provide the right solutions for it. We can make solutions before it is too late. When a person starts to have struggles with his thoughts, and can notice unusual behavior with himself, it is time for him to seek help before the problem gets worse. It is not usual to have unusual attitudes, so we have to take a psychological test to ensure that our mental health is not in danger. Aside from these things, a psychological assessment is needed in different situations like as evidence in the court or a test that we should take in the recruitment process in an employment. When our behaviour is needed to be examined, we have to undergo a psychological assessment. It is not bad. We will know the extent of our behaviour and we can be released with the mental stress. We can know if we have a mental problem or not.
What is the assessment of a patient in nursing?
Nursing assessment includes emotional and mental assessment, physical assessment , and environmental and social issues that affect the patient’s health. It is important that the nurses should evaluate and observe for these factors to properly assist the patient and give immediate medications to the health problems encounter by patients.
What is physical assessment in nursing?
Physical Assessment in Nursing. Physical assessment is the structured examination perform by the nurse to collect the complete data about the patient. The techniques that nurses used in this kind of health assessment examinations are; observation, inspection, palpation, percussion, and auscultation. Physical assessment information includes:
What Is a Nursing Assessment?
Nursing assessment is the systematic and dynamic examination that allows the nurse to gather and analyze the information about the patient’s physiological, psychological, sociological, spiritual, economic and lifestyle status.
What does a nurse do when a patient refuses to eat?
Not only a nurse will conduct the patient’s assessment of the physical causes and manifestation of pain, but also the response of the patient, this includes the patient’s refusal to eat, the failure of getting out of bed, anger towards the health staff, fear of dying, fatigue, and the request for pain medication.
What is the purpose of a health assessment?
The purpose of this assessment is to evaluate the patient’s resources and strengths and to identify the health status and health problems which can be used during service planning and to provide a detailed database that is crucial in evaluating changes in the patient’s health.
What to check for when you have a bone fracture?
Check if the bones have deformities, tenderness, and swelling.
Can an unauthorized nurse perform a nursing assessment?
Unauthorized personnel can not, will not, and are not allowed to perform the nursing assessment, it should only be the registered nurse.
Popular Posts:
- 1. patient portal pending
- 2. the nurse caring for a 90 year old patient with a closed head injury would immediately report:
- 3. watson clinic main patient portal
- 4. what creates recent searces on intelichart patient portal
- 5. custom patient portal solution
- 6. can a do tor report a patient to the cdc without results from a specimen first
- 7. fcne patient portal'
- 8. dr jay williamson patient portal
- 9. patient portal neuromedical center
- 10. mayoclinic patient my chart login