Ems Patient Care Report Form - signNow
14 hours ago Patient Care; Why You Need the EMS Run Report. By. Bryan Bledsoe, DO, FACEP, FAAEM, EMT-P-1.31.2010. Facebook. ... This is where the EMS run report comes into play. Critical Information >> Go To The Portal
How do I obtain a patient’s signature for Medicare claim submission purposes?
For Medicare claim submission purposes, there are numerous ways to obtain a patient’s signature for claim submission purposes, including: Patient representatives (guardians, POA, family members, even facility representatives who previously cared for the transport)
Why did the owner remove the patient’s ambulatory status?
Specifically, the owner removed all references to the patients’ ambulatory status, in order to help establish the need for ambulance. This case also involved significant penalties and a jail sentence for the owner.
What happens if a crewmember signs a patient’s name without consent?
A crewmember signing a patient’s name without the patient’s consent meets the legal definition of forgery. The potential penalty for fraud lies with the perpetrator.

How do I write a patient care report in EMS?
EMS providers just need to pull the information together and write it down in a way that paints a picture....Follow these 7 Elements to Paint a Complete PCR PictureDispatch & Response Summary. ... Scene Summary. ... HPI/Physical Exam. ... Interventions. ... Status Change. ... Safety Summary. ... Disposition.
What is a run report EMS?
Emergency respondents should develop a system for writing reports so the run sheets are thorough but concise every time. Gather information on the medical emergency, noting what type of incident caused the injury, the estimated age and sex of the victim, and his condition at the scene.
What are the components of a patient care report?
Patients name and the chief complaint, nature of the illness, or mechanism of injury. Detailed information, such as pertinent negatives and findings of a more detailed physical exam. Any medical history not already given. The patient's response to treatment given en route.
What information should your handoff report to the paramedics include?
The handoff report to paramedics should include a full nursing report but can omit items such as last bowel movement and ambulatory status, unless they're relevant to the transport.
What is a run report?
Run report means the standard report form developed by the Commissioner to facilitate the collection of a standardized data set related to the provision of emergency medical and trauma care in accordance with 63 O.S. Section 1-2511.
What is on an EMS run form?
The trip/run sheet of the patient's encounter is used as a medical record for ambulance services and should include the following: Complete and legible information. Every page of the record must be legible and include the appropriate patient information (e.g., complete name, dates of service).
How do you write a patient report?
III. Patient case presentationDescribe the case in a narrative form.Provide patient demographics (age, sex, height, weight, race, occupation).Avoid patient identifiers (date of birth, initials).Describe the patient's complaint.List the patient's present illness.List the patient's medical history.More items...•
What does soap mean in EMS?
Subjective, Objective, Assessment and PlanIntroduction. The Subjective, Objective, Assessment and Plan (SOAP) note is an acronym representing a widely used method of documentation for healthcare providers. The SOAP note is a way for healthcare workers to document in a structured and organized way.[1][2][3]
Which is run data on a PCR?
What is "run data?" This includes the agency name, unit number, date, times, run or call number, crew members' names, licensure levels, and numbers. Remember -- the times that you record must match the dispatcher's times.
How do I give a good handoff report to EMS?
0:185:41Patient Handoff Report Skills | EMT | V28 - YouTubeYouTubeStart of suggested clipEnd of suggested clipHaving an organized or systematic approach to patient handoff reports is a great way to get startedMoreHaving an organized or systematic approach to patient handoff reports is a great way to get started in practice.
What is EMS handoff?
The patient's vital signs are reportedly within normal limits, so she is triaged to a regular room in the emergency department where handoff is given from paramedic to nurse. The physician, who is in another room, is not present for the signout. Ten minutes later, the physician walks into the room to see the patient.
What is a radio report?
Radio reporting (Beginner/Advanced) Radio news reports allow the listener to find themselves at the heart of the action, to hear noises, to get a grasp of surroundings. To achieve this, a reporter must paint a picture in the listener's mind through commentary, interviews and describing the atmosphere at the scene.
How do you write a good EMS narrative?
How to Write an Effective ePCR NarrativeBe concise but detailed. Be descriptive in explaining exactly what happened and include the decision-making process that led to the action. ... Present the facts in clear, objective language. ... Eliminate incorrect grammar and other avoidable mistakes. ... Be consistent and thorough.
What is the prehospital care report?
(prē-hos'pi-tăl kār rĕ-pōrt') An electronic or written report completed by a prehospital provider that contains demographic and medical information as well as a record of the treatment and transport of a patient.
Why is documentation important in EMS?
The primary purpose of EMS documentation is to provide a written record of patient assessment and treatment that can help guide further care. For the information to be readily understood and communicated, it must be organized in a format that all healthcare providers involved in patient care will understand.
What is pertinent negative?
Pertinent Negatives (PN) are used when the clinician documents why they DID NOT perform a procedure. Example: If Aspirin is part of the agency protocol for Chest Pain but was not administered, the reason should be documented. This is done using PN values.
1. Facts surrounding the dispatch undocumented
Many times when an ambulance responds to a 911 call, that simple fact is missing from the ePCR. And in way too many chart reviews or audits, we find no dispatch determinants or other clear indication of the patient’s reported condition at the time of dispatch.
3. Vague explanation of specific interventions and procedures performed
Too many times we find nothing more than "per protocol" to explain why a cardiac monitor was applied, an IV was initiated or some other procedure was performed. Just like the ambulance service must be medically necessary to be reimbursed by Medicare and other payers, the treatments provided must also be medically necessary.
4. No explanation for EMS-specific care and treatment
This is important with regard to two areas. First, is clearly explaining the transport itself and the service or care the patient required during the transport that could not be provided other than by trained medical professionals in an ambulance.
5. Inadequate description of patient complaints or findings
The most common example of an inadequately described or quantified complaint or finding is with regard to a patient's pain.
About the author
For over 20 years, PWW has been the nation’s leading EMS industry law firm. PWW attorneys and consultants have decades of hands-on experience providing EMS, managing ambulance services and advising public, private and non-profit clients across the U.S.
Why is it important to have a signature on an EMS report?
That should appear immediately under the signature line. This is especially important when the signature of the person completing the report is illegible. It also helps to ensure continuity of care, and that the assessment and treatment was provided by properly certified EMS practitioners in accordance with your state’s EMS laws.
What is legibly signing your patient care reports?
The bottom line is that legibly signing your patient care reports, including your printed name and credentials, is a fundamental standard of care for PCR completion and an essential part of being a healthcare professional. No posts to display.
What is Medicare program integrity manual?
Specifically, the Medicare Program Integrity Manual, chapter 3, section 3.3.2.4 states, “Medicare requires that services provided/ordered/certified be authenticated by the persons responsible for the care of the beneficiary.”.
Do all EMS crew members sign PCR?
In most states , the EMS laws don’t expressly state that all crew members must sign the PCR. Usually, laws require the primary caregiver to complete the PCR. However, having all crew members sign the PCR is a standard for EMS documentation that should be followed for three primary reasons.
Is it good to sign a PCR?
Second, it’s simply good medical care for all crew members to sign the PC R. Healthcare is all about accountability and transparency. Even if you’re not the primary care provider, you participated in the patient encounter. When providing medical care, everyone involved with the patient must be accountable for the care they provide, and all crew members should sign the PCR if you want to call it a complete medical record.
Can PCR be signed electronically?
Your signature can be handwritten as part of a paper report, or the report can be signed electronically. Most electronic PCR solutions have effective ways of capturing your actual digital signature with a stylus, or your typed name as an electronic signature. Electronic signatures will suffice as long as there are proper login ...
Thanks for joining us!
Today marks the first in our Documentation 101 blog series. Using the next several blog postings, we’ll be attempting to put together a few coaching blogs to help all of you become better EMS documenters.
Maybe you need some basic writing help?
There’s nothing wrong in admitting that you need help. You can even better yourself, personally, by learning to communicate in writing more effectively. There are tons of self-help tools on the Internet to assist you with writing and grammar skills.
To the Rescue!
We’re not finished. As part of this documentation series, we’ll include some specific steps to make you a better documenter. Make your goal to be the best documenter that your department has and you’re well on your way to PCR writing success.
Not a client?
No problem there. Check out our website right now and complete the “Get Started” section so we can connect. We’d love to talk to you about the many features and how they can benefit your EMS Department!
Why did the owner remove references to the patients' ambulatory status?
Specifically, the owner removed all references to the patients’ ambulatory status, in order to help establish the need for ambulance. This case also involved significant penalties and a jail sentence for the owner.
What is a patient representative?
Patient representatives (guardians, POA, family members, even facility representatives who previously cared for the transport) A combination of crew and receiving facility representatives acknowledging the patient was unable to sign and that none of the other representatives were willing or available to sign.
Can ALS be fraudulently billed?
That is, a crewmember can document that ALS care was provided (when it was really not), but if the claim is not billed at all, or only billed at the BLS level (and all coverage criteria for insurance are met), then there would likely be no fraudulent billing.
Is a forged signature a fraud?
If a crewmember forges someone else’s signature and a biller relies on that forged signature when billing insurance, it can become a fraudulent billing case, similar to those referenced above. But, the forged signature alone is also fraudulent. For example, in Pennsylvania, “a person is guilty of forgery if ...
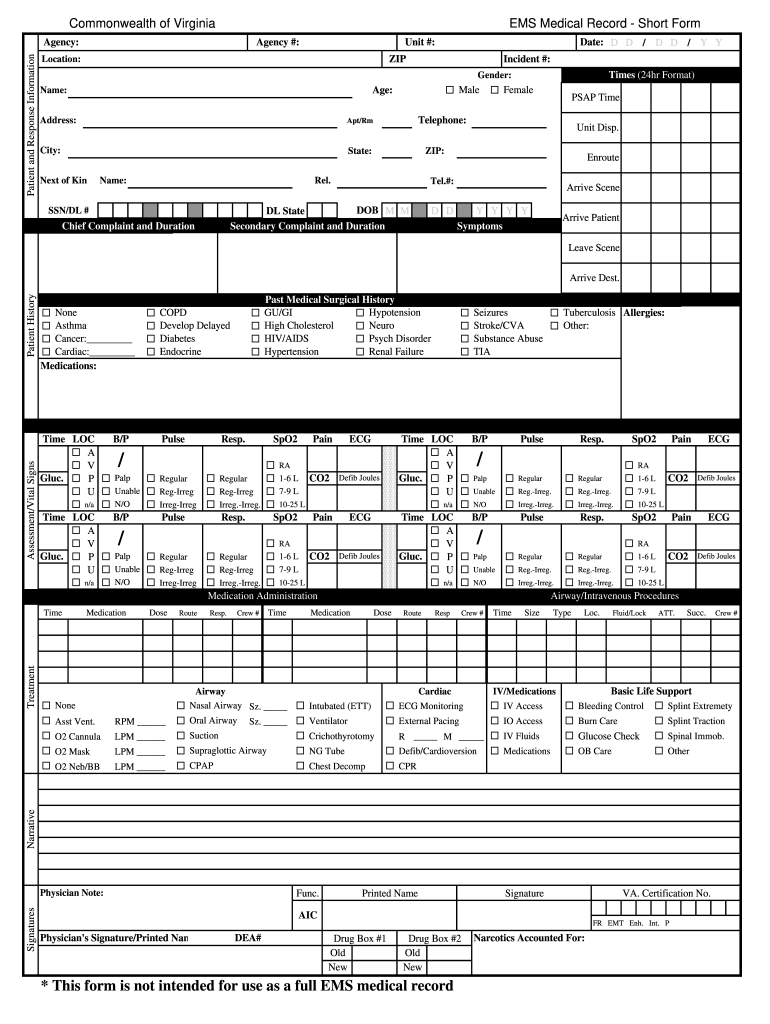
Paper Patient Care Report (PCR)
Here is an example of two versions of print out, paper PCR you can download and use in your service.
Electronic Patient Care Report (ePCR)
The state of Alaska provids a free ePCR (Electronic Patient Care Report) system allowing communities to customize their run report forms to match their specific community needs.
Facts Surrounding The Dispatch Undocumented
Insufficient Narrative of The Patient’S Condition at The Time of Transport
- Far too frequently we see PCR narratives that do little more than state where the patient was picked up from, where they were delivered to and some statement that indicates that the crew left the patient no worse off than they found them — such as, "patient transported without incident." This is especially true in the case of non-emergency transports. For every transport, whether em…
Vague Explanation of Specific Interventions and Procedures Performed
- Too many times we find nothing more than "per protocol" to explain why a cardiac monitorwas applied, an IV was initiated or some other procedure was performed. Just like the ambulance service must be medically necessary to be reimbursed by Medicare and other payers, the treatments provided must also be medically necessary. Interventions and procedures should be …
No Explanation For Ems-Specific Care and Treatment
- This is important with regard to two areas. First, is clearly explaining the transport itself and the service or care the patient required during the transport that could not be provided other than by trained medical professionals in an ambulance. Second, in the case of a patient being transported from one facility to another, what specific service...
Inadequate Description of Patient Complaints Or Findings
- The most common example of an inadequately described or quantified complaint or finding is with regard to a patient's pain. EMTs and paramedics should always describe a finding or complaint of pain by documenting completely the Onset, Provocation, Quality, Radiation, Severity and Time (OPQRST), as well as the patient's pain rating on a scale of zero to 10. The word "pain" …
Popular Posts:
- 1. regional orthopedic associates patient portal
- 2. bailey square patient portal
- 3. los coyotes imaging patient portal
- 4. patient keeper medical access portal
- 5. abinton health patient portal
- 6. patient portal creekside medical
- 7. patient portal pediatric care specialists
- 8. dr hubbly patient portal
- 9. what possible side effect should a patient taking tadalafil report to a physician quizlet
- 10. mt ascutney patient portal