How to write a better EMT patient care report - EMS1
1 hours ago EMS Patient Care Report Writing | Documentation 101 | Part 4c - Dispatch - BLS Level of Service & Routine Transports Welcome to Part 4c in our continuing blog series "EMS Patient Care Reporting Writing/Documentation 101" Part 1: EMS Patient Care Report … >> Go To The Portal
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the information necessary for the assessment and evaluation of a patient’s care.
Full Answer
How do you write a patient care report?
- Recognition and description of a new disease
- Recognition of rare manifestations of a known disease
- Elucidation of the mechanisms of a disease
- Detection of adverse or beneficial side effects of drugs (and other treatments)
- Medical education and audit
Why do you need the EMS run report?
Prehospital Care Reports
- PCR/ePCR Use: A PCR/ePCR should be completed each time the EMS agency is dispatched for any type response. ...
- Information Entry: All information written on the paper PCR should be legible and printed in blue or black ink. ...
- Distribution of Paper PCRs: Ambulance Service: Leave the "pink" copy at the hospital prior to the agency leaving the hospital. ...
How to improve EMS patient handoffs at emergency department?
- Study objective. Patient handoffs are known as high-risk events for medical error but little is known about the professional, structural, and interpersonal factors that can affect the patient transition from ...
- Methods. ...
- Results. ...
- Conclusion. ...
How to write a better EMT patient care report?
- Each PCR should include all pertinent times associated with the EMS call.
- As well as the times of the assessments and treatments provided, the PCR should include detailed signs and symptoms and other assessment findings such as vital signs, and all the ...
- Also documented are changes in patient condition after treatment.
How do I write an EMS patient care report?
EMS providers just need to pull the information together and write it down in a way that paints a picture....Follow these 7 Elements to Paint a Complete PCR PictureDispatch & Response Summary. ... Scene Summary. ... HPI/Physical Exam. ... Interventions. ... Status Change. ... Safety Summary. ... Disposition.
What is a EMS report?
The primary purpose of EMS documentation is to provide a written record of patient assessment and treatment that can help guide further care. For the information to be readily understood and communicated, it must be organized in a format that all healthcare providers involved in patient care will understand.
What should be included in a patient care report?
What Patient Care Reports Should IncludePresenting medical condition and narrative.Past medical history.Current medications.Clinical signs and mechanism of injury.Presumptive diagnosis and treatments administered.Patient demographics.Dates and time stamps.Signatures of EMS personnel and patient.More items...•
What is patient assessment EMS?
Steps taken by EMS providers when approaching the scene of an. emergency call; determining scene safety, taking BSI precautions, noting the mechanism of injury or patient's nature of illness, determining the number of patients, and deciding what, if any additional resources are needed including Advanced Life Support.
What is a patient report?
A patient report is a medical report that is comprehensive and encompasses a patient's medical history and personal details. It's often written when they go to a health service provider for a medical consultation. Government or health insurance providers may also request it if they need it for administration reasons.
What is EMS documentation?
First and foremost, EMS documentation serves a vital clinical purpose. It is the record of your assessment and care of patients. It becomes part of the patient's medical record, both at the receiving facility and within your EMS organization.
How do you write a patient report?
III. Patient case presentationDescribe the case in a narrative form.Provide patient demographics (age, sex, height, weight, race, occupation).Avoid patient identifiers (date of birth, initials).Describe the patient's complaint.List the patient's present illness.List the patient's medical history.More items...•
How do you take care of a patient report?
Document the patient's history completely. Remember bystanders or those close to the patient can often provide valuable information about the patient....Check descriptions. ... Check (and recheck) spelling and grammar. ... Assess your chief complaint description. ... Review your impressions. ... Check the final details.
How do you write a PT report?
Summary: The format of a patient case report encompasses the following five sections: an abstract, an introduction and objective that contain a literature review, a description of the case report, a discussion that includes a detailed explanation of the literature review, a summary of the case, and a conclusion.
What are the 5 primary assessments?
the six parts of primary assessment are: forming a general impression, assessing mental status, assessing airway, assessing breathing, assessing circulation, and determining the priority of the patient for treatment and transport to the hospital.
How do you assess patient status?
Patient assessment commences with assessing the general appearance of the patient. Use observation to identify the general appearance of the patient which includes level of interaction, looks well or unwell, pale or flushed, lethargic or active, agitated or calm, compliant or combative, posture and movement.
How do you perform a patient assessment?
WHEN YOU PERFORM a physical assessment, you'll use four techniques: inspection, palpation, percussion, and auscultation. Use them in sequence—unless you're performing an abdominal assessment. Palpation and percussion can alter bowel sounds, so you'd inspect, auscultate, percuss, then palpate an abdomen.
What is BLS in dispatch?
If your department is a Basic Life Support (BLS) service then your recording of the nature of dispatch serves two purposes, unlike the company that must justify ALS versus BLS and assuming that your company does not joint bill with an ALS provider.
Is a scheduled or non-scheduled flight a non-emergency?
One of the key items to call to your attention is the fact that a non-emergency/routine, scheduled or non-scheduled stays a non-emergency for billing purposes even if the incident becomes serious during transport.
Thanks for joining us!
Today marks the first in our Documentation 101 blog series. Using the next several blog postings, we’ll be attempting to put together a few coaching blogs to help all of you become better EMS documenters.
Maybe you need some basic writing help?
There’s nothing wrong in admitting that you need help. You can even better yourself, personally, by learning to communicate in writing more effectively. There are tons of self-help tools on the Internet to assist you with writing and grammar skills.
To the Rescue!
We’re not finished. As part of this documentation series, we’ll include some specific steps to make you a better documenter. Make your goal to be the best documenter that your department has and you’re well on your way to PCR writing success.
Not a client?
No problem there. Check out our website right now and complete the “Get Started” section so we can connect. We’d love to talk to you about the many features and how they can benefit your EMS Department!
What Is a Patient Care Report?
We often hear of care reports based on by medical teams or by medical authorities. Yet, we are not sure how this differs from the kind of report that is given to us by the same people. So this is the time to make it as clear as possible.
How to Write a Patient Care Report?
Where do you even begin when you write a patient care report? A lot of EMS or EMTs do know how to write one since they are trained to do so.
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the information necessary for the assessment and evaluation of a patient’s care.
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very careful and very meticulous when writing these kinds of reports. Every detail counts.
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make sure that you have all the information correctly. One wrong information can cause a lot of issues and problems.
When did Rob DeMeo become a paramedic?
When Rob DeMeo became a paramedic in 2003, the last thing he was concerned about was writing a patient care report (PCR). "We had maybe one hour on documentation in class," the New York native recalls.
What is ePCR in medical?
Electronic patient care reporting , more commonly known as ePCR, is rapidly replacing the paper forms many of us still use. ePCR not only improves the accuracy and legibility of documentation, but also allows EMS providers to sort and summarize prehospital data in many ways.
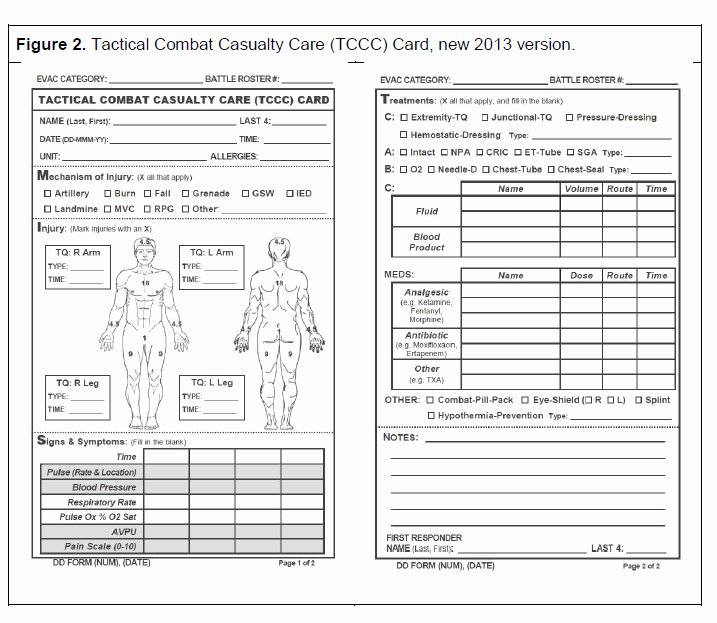
Paper Patient Care Report (PCR)
Here is an example of two versions of print out, paper PCR you can download and use in your service.
Electronic Patient Care Report (ePCR)
The state of Alaska provids a free ePCR (Electronic Patient Care Report) system allowing communities to customize their run report forms to match their specific community needs.

Be Specific
Paint A Picture of The Call
- The PCR must paint a picture of what happened during a call. The PCR serves: 1. As a medical record for the patient, 2. As a legal record for the events that took place on the call, and 3. To ensure quality patient care across the service. PCRs should go beyond merely stating that a patient was picked up at a certain location, transported to another location and that the transpor…
Do Not Fall Into Checkbox Laziness
- EMS professionals have long been promised a PCR that basically writes itself. Electronic PCR softwareis a great tool and can improve the efficiency of PCR completion. However, simply clicking a box or making a selection from a drop-down menu cannot be a substitute for your words in the form of a clear, concise, accurate and descriptive clinical narrative. An EMS provide…
Complete The PCR as Soon as Possible After A Call
- Most states, and many EMS agencies themselves, often have time limits within which the PCR must be completed after the call ended – 24, 48 or 72 hours are common time limits. While it is always important to comply with time limits, there are benefits to getting your PCR completed as soon as possible – preferably right after the call is completed an...
proofread, proofread, Proofread
- The easiest way to improve your PCR is to proofread before submitting it. We understand the dilemma, after writing the sixth PCR for the day, and having 10 minutes left in the shift, the last thing anyone wants to do is sit there and reread what they have just written. But that is exactly what needs to be done. Poor grammar and spelling is the easiest way to have your abilities calle…
Popular Posts:
- 1. estrella ent patient portal
- 2. upmc kane patient portal
- 3. patient safety report to congress
- 4. patient is diagnosed with diabetic cataract. report code(s):
- 5. maxwell group patient portal
- 6. center for behavioral health middletown ct patient portal
- 7. rex family practice knightdale patient portal
- 8. privia medica group patient portal
- 9. patient portal prohealthcare
- 10. frye care patient portal