Coccidioides immitis and posadasii; A review of their …
10 hours ago Coccidioides immitis and C. posadasii are two highly pathogenic dimorphic fungal species that are endemic in the arid areas of the new world, including the region from west Texas to southern and central California in the USA that cause coccidioidomycosis (also known as Valley Fever). In highly endemic regions such as southern Arizona, up to 50% ... >> Go To The Portal
What is Coccidioides immitis and C posadasii?
Coccidioides immitis and C. posadasii are two highly pathogenic dimorphic fungal species that are endemic in the arid areas of the new world, including the region from west Texas to southern and central California in the USA that cause coccidioidomycosis (also known as Valley Fever). In highly endem …
How can we rule out Coccidioides (cocci) and Cryptococcus?
Serology and fungal cultures were sent to rule out fungi such as Coccidioides (Cocci) and Cryptococcus. Serology for Coccidioides consist of enzyme immunoassay, immunodiffusion and complement fixation. All serologies were positive for Coccidioides. The cultures were also positive from lung samples taken from the patient.
What is Coccidioides meningitis?
The patient was diagnosed with disseminated Coccidioides, Coccidioides pneumonia and Coccidioides meningitis. Coccidioides is the causative agent of Coccidioidomycosis, also known as Valley Fever, which gets its name from the San Joaquin Valley in California. The organism is a dimorphic fungus that exists in the soil.
What is the causative agent of Coccidioides pneumonia?
The patient was diagnosed with disseminated Coccidioides, Coccidioides pneumonia and Coccidioides meningitis. Coccidioides is the causative agent of Coccidioidomycosis, also known as Valley Fever, which gets its name from the San Joaquin Valley in California.
What was the finding of MRI in April 2014?
Findings from MRI in April 2014 included a large joint effusion, severe synovitis, large cortical erosions and loss of cartilage. Oedema was described in the posterior compartment muscles, and a 2.2 cm soft tissue mass was seen in the anterior-medial soft tissues.
What causes coccidioidomycosis?
Coccidioidomycosis is caused by the dimorphic fungi Coccidioides immitis, and C. posadasii. Over half of infections are asymptomatic. Among symptomatic patients, the most common presentation is an acute pneumonia often with headache and fatigue. 1 A minority of symptomatic patients require antifungal treatment. Bone and joint infection with Coccidioides can occur and represents disseminated disease. 2 3 Optimal treatment of Coccidioides septic arthritis is not defined in recent guidelines. 4 Surgical treatment is often recommended, 5 though some experts find that infection limited to the synovium can be treated medically. 6 We present a case where aggressive surgical and medical therapy were necessary to obtain a good long-term outcome.
What is C. posadasii meningoencephalitis?
We report a case of C. posadasii meningoencephalitis in a previously healthy 42-year-old Caucasian male who returned to Canada after spending time working in New Mexico. He presented with a 3-week history of headache, malaise and low-grade fevers. He developed progressive confusion and decreasing level of consciousness following hospitalization. Evidence of hydrocephalus and leptomeningeal enhancement was demonstrated on magnetic resonance imaging (MRI) of his brain. Serologic and PCR testing of the patient's CSF confirmed Coccidioides posadasii. Despite appropriate antifungal therapy he continues to have significant short-term memory deficits and has not returned to his full baseline functional status.
What are the two most common diseases in humans?
Two species cause most human disease: Coccidioides immitis (primarily California isolates) and Coccidioides posadasii. Coccidioidomycosis is typically acquired through inhalation of soil or dust containing spores. Coccidioidal meningitis (CM), most common in the immunocompromised host, can also affect immunocompetent hosts.
Which fungi cause human disease?
Background. Coccidioides species are dimorphic fungi within the Ascomycete division [ 1 ]. The two species that have been found to cause human disease are Coccidioides immitis and Coccidioides posadasii [ 2, 3 ]. C. immitis and C. posadasii are morphologically identical with no known phenotypic differences in pathogenicity.
Where are C. immitis and C. posadasii found?
immitis being found predominantly in California and C. posadasii in Nevada, Arizona, New Mexico, Texas, Central and South America [ 2, 3, 4, 5, 6 ].
How long can arthroconidia be in the soil?
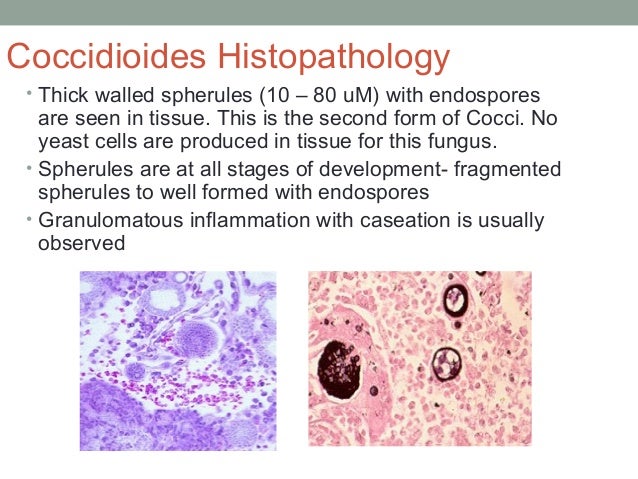
Arthroconidia can remain viable in soil for years and can be released into the air through soil disruption [ 1, 5 ]. Inhalation of arthroconidia leads to infection by conversion into spherules within the susceptible host. The spherules rupture, releasing endospores into surrounding tissues, producing more spherules [ 1, 5 ].
Does travel to endemic regions cause disease?
Travel to endemic regions can result in disease secondary to Coccidioides spp. and requires physicians in non-endemic areas to have a high index of suspicion. Effective therapeutic options have reduced the mortality rate of CM, however, it is still associated with significant morbidity and requires life-long therapy.
Presentation
A 62-year-old male presents to the emergency department with complaints of fever, headache and altered mental status. The patient has a history of Type 2 Diabetes, hypertension, high cholesterol and had been treated a month prior for pneumonia and persistent cough.
Lab Testing
Serology and fungal cultures were sent to rule out fungi such as Coccidioides (Cocci) and Cryptococcus. Serology for Coccidioides consist of enzyme immunoassay, immunodiffusion and complement fixation. All serologies were positive for Coccidioides. The cultures were also positive from lung samples taken from the patient.
Cause of Symptoms
The patient’s occupation as a construction worker exposed him to the environmental spores of Coccidioides. The patient was diagnosed with disseminated Coccidioides, Coccidioides pneumonia and Coccidioides meningitis.
Treatment
Mild to moderate disease is treated with either Fluconazole or Itraconazole. Severe disease (with rapid progression and/or infection of critical organs) is treated with Liposomal Amphotericin B. Other alternative therapies exist.