Ems Patient Care Report Form - Fill Out and Sign …
26 hours ago How to complete the Report form patient care form on the web: To get started on the document, use the Fill camp; Sign Online button or tick the preview image of the form. The advanced tools of the editor will direct you through the editable PDF template. Enter your official identification and contact details. Apply a check mark to indicate the ... >> Go To The Portal
How do I create a patient care report template?
Utilize a check mark to indicate the answer where required. Double check all the fillable fields to ensure complete precision. Make use of the Sign Tool to create and add your electronic signature to signNow the Patient care report template form. Press Done after you finish the form. Now you'll be able to print, save, or share the document.
What is a patient care report in EMS?
An often underrepresented skill that EMS staff need to work on is writing detailed patient care reports (PCRs) that provide a clear clinical picture of the patient's needs. ... For many EMS services, the bulk of revenue comes from insurance reimbursements. What is included in a patient care report?
What are the parts of a patient report form?
The Parts of Patient Report Forms In completing the patient report forms, below are the following important or essential information that should be provided. Otherwise, results from medical assessments cannot be given due to deficiency of relevant information. The patient’s personal information The patient’s full name The date of birth The gender
Why are nursing report templates important in healthcare?
This means that, even if there is a change in the shifts of a particular group of doctors or nurses, the subsequent shift can continue providing care to their patients without any obstacles. Being such a useful and essential part in healthcare circles, these nursing report templates are implemented by institutions all around the world.

How do you write a patient care report?
There are seven elements (at a minimum) that we have identified as essential components to documenting a well written and complete narrative.Dispatch & Response Summary. ... Scene Summary. ... HPI/Physical Exam. ... Interventions. ... Status Change. ... Safety Summary. ... Disposition.
How do you write a good PCR?
How to Write an Effective ePCR NarrativeBe concise but detailed. Be descriptive in explaining exactly what happened and include the decision-making process that led to the action. ... Present the facts in clear, objective language. ... Eliminate incorrect grammar and other avoidable mistakes. ... Be consistent and thorough.
How do you fill out a PCR EMT?
0:1915:38Patient Care Report Edition 3, Completion Guide - YouTubeYouTubeStart of suggested clipEnd of suggested clipWithout having to open it. Out.MoreWithout having to open it. Out.
What is a PCR document?
The PCR documentation is considered a medical document that becomes part of the patient's permanent medical record. It is also considered a legal document in cases where liability and/or malpractice issues arise. It is the source in which all medical billing claims are based.
What is the primary purpose of a patient care report?
The primary purpose of the Patient Care Report (PCR) is to document all care and pertinent patient information as well as serving as a data collection tool.
When you document information on a patient that you treat and care for this written report is called the?
When you document information on a patient that you treat and care for. This written report is called the: Patient care report, run report.
How do you write a patient narrative in EMS?
1:3211:38How to Write a Narrative in EMS || DCHART Made Easy ... - YouTubeYouTubeStart of suggested clipEnd of suggested clipSection some people include a lot less some people will just include the reference. And the address.MoreSection some people include a lot less some people will just include the reference. And the address. So next is the chief complaint. And this is pretty self-explanatory.
What is a patient care form?
Patient care report or “PCR” means a report that documents the assessment and management of the patient by the emergency care provider.
What information is patient data on a PCR?
What is a primary difference in the type of information found in the administrative section and in the patient information section of the PCR? A. The patient information includes the patient's address only and the administrative section includes the trip times.
What is an example of PCR?
PCR allows specific target species to be identified and quantified, even when very low numbers exist. One common example is searching for pathogens or indicator species such as coliforms in water supplies.
What does PCR stand for in healthcare?
PCR (polymerase chain reaction) tests are a fast, highly accurate way to diagnose certain infectious diseases and genetic changes. The tests work by finding the DNA or RNA of a pathogen (disease-causing organism) or abnormal cells in a sample.
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the inf...
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very caref...
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make...
The way to fill out the Patient care report template form on the internet
To get started on the blank, utilize the Fill & Sign Online button or tick the preview image of the form.
Video instructions and help with filling out and completing Patient Care Report Template Doc Form
Find a suitable template on the Internet. Read all the field labels carefully. Start filling out the blanks according to the instructions:
Instructions and help about health care report template
the aim of this audio-visual presentation is to provide clear guidance for the accurate completion of the patient care report recording pre-hospital care interventions and medications administered to patients is an essential clinical responsibility of all pre-hospital emergency care practitioners every responder and practitioner must provide clear accurate and comprehensive patient care information the PCR is a two-part pocket-sized report comprising 10 colored panels and folded in such a way that the written information flows easily from panel to panel without having to open it out on the Topkapi the following is recorded incident information patient demographic information clinical information vital observations medication treatment care management continuity of care clinical audit emergency department handover signature and additional information the second copy has four additional panels on the back for use by the practitioner to record the following out of hospital cardiac arrest.
FAQs ems patient care report template
Here is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Why are patient forms at hospitals such a pain to fill out?
Usually there is a one or maybe a two-page form. I don't think they are that difficult to fill out. They copy my insurance card and that's it. Generally they include a brief list of history questions and current symptom questions. If it is a current doctor, only the current symptom questions.
What tax forms do I need to fill out for reporting bitcoin gains and loses?
IRS1040 and 1099 forms.“For instance, there is no long-term capital gains tax to pay if you are in the lower two tax brackets (less than $36,900 single income or less than $73,800 married income).
Do military members have to pay any fee for leave or fiancee forms?
NOOOOOOO. You are talking to a military romance scammer.
How to Edit Your Ems Pcr Template Pdf Form Online
When you edit your document, you may need to add text, fill in the date, and do other editing. CocoDoc makes it very easy to edit your form with the handy design. Let's see how to finish your work quickly.
How to Edit Text for Your Ems Pcr Template Pdf Form with Adobe DC on Windows
Adobe DC on Windows is a popular tool to edit your file on a PC. This is especially useful when you finish the job about file edit without using a browser. So, let'get started.
How to Edit Your Ems Pcr Template Pdf Form With Adobe Dc on Mac
Find the intended file to be edited and Open it with the Adobe DC for Mac.
How to Edit your Ems Pcr Template Pdf Form from G Suite with CocoDoc
Like using G Suite for your work to sign a form? You can make changes to you form in Google Drive with CocoDoc, so you can fill out your PDF without worrying about the increased workload.
What Is a Patient Care Report?
We often hear of care reports based on by medical teams or by medical authorities. Yet, we are not sure how this differs from the kind of report that is given to us by the same people. So this is the time to make it as clear as possible.
How to Write a Patient Care Report?
Where do you even begin when you write a patient care report? A lot of EMS or EMTs do know how to write one since they are trained to do so.
What is a patient care report?
A patient care report is a document made mostly by the EMS or EMTs. This documented report is done after getting the call. This consists of the information necessary for the assessment and evaluation of a patient’s care.
What should not be written in a patient care report?
What should be avoided in a patient care report is making up the information that is not true to the patient. This is why you have to be very careful and very meticulous when writing these kinds of reports. Every detail counts.
Who is in charge of reading the patient care report?
The person or the people who will be reading the report are mostly medical authorities. When you are going to be passing this kind of report, make sure that you have all the information correctly. One wrong information can cause a lot of issues and problems.
Birmingham Regional Emergency Medical Services System
Real-time EMS serving Blount, Chilton, Jefferson, Shelby, St. Clair, Walker, & Winston counties in North Central Alabama.
410 10th Ave South, Suite B, Birmingham, AL 35205
Effective September 1, 2021, the BREMSS administrative offices and classroom facilities have moved to our new location.
The NREMT has waived limits on Distributive Education for 2022!
We will not be conducting a live course prior to the March 31, 2022 renewal date. To access our distributive NCCR refresher go to the BREMSS eLearning home and request access to our Learning Management System.
Birmingham Regional Emergency Medical Services System
Real-time EMS serving Blount, Chilton, Jefferson, Shelby, St. Clair, Walker, & Winston counties in North Central Alabama.
410 10th Ave South, Suite B, Birmingham, AL 35205
Effective September 1, 2021, the BREMSS administrative offices and classroom facilities have moved to our new location.
What is the relevant information needed for a patient complaint?
In a patient complaint, the relevant information that are needed are as follows: The description of the situation. The effect on privacy.
Why are patient reports important?
Why Patient Reports Are Needed. Patient medical reports serve as evidences that the patient has been given proper medications or treatments. Doctors or physicians are doing the best they could in order to supply the needs of each and every patient, regardless if they are in a critical condition or not.
What is healthcare personnel?
Healthcare personnel in hospitals or medical centers ensure that they provide the needs of the patients (pertaining to the treatments or medications needed) and their individual relatives (pertaining to the answers or provision of exact details from the medical results). It goes without saying that everyone wants an accurate general information ...
Do hospitals keep records of patients?
Therefore, it is mandatory that the medical clinic, center, or hospital keeps a record of their patients. These patient reports also help the doctors and the relatives of the patient to know what is or are behind the patients’ results of their individual health assessment.
Can results from medical assessments be given due to deficiency of relevant information?
Otherwise, results from medical assessments cannot be given due to deficiency of relevant information.
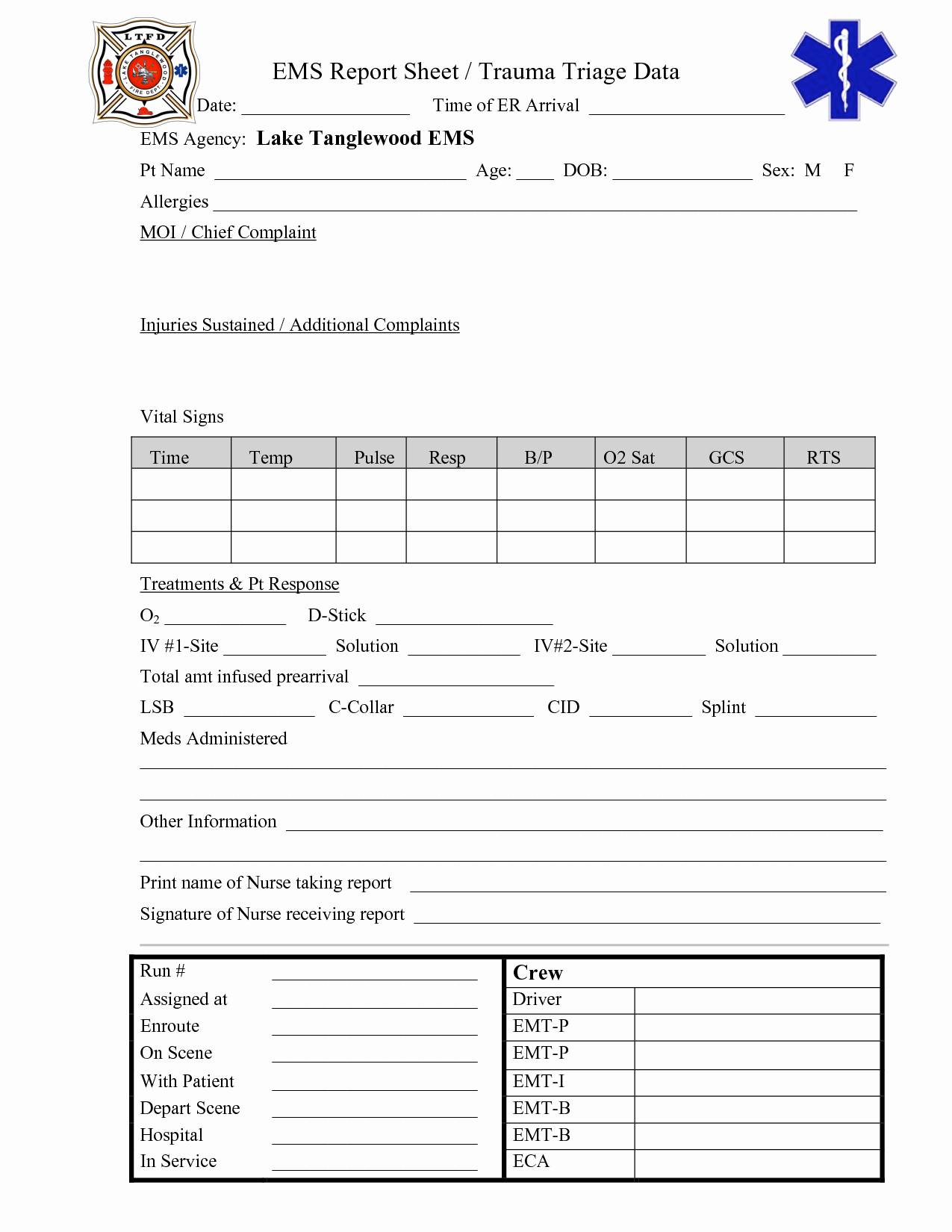
Paper Patient Care Report (PCR)
Here is an example of two versions of print out, paper PCR you can download and use in your service.
Electronic Patient Care Report (ePCR)
The state of Alaska provids a free ePCR (Electronic Patient Care Report) system allowing communities to customize their run report forms to match their specific community needs.
What is a nursing report sheet?
The report sheets enable the nurses to record clear information regarding details including the diagnosis, history, allergies, consults, vital signs, lab results, and other such health-related data. Due to their excellent recording system, nursing report sheets are used by physicians, doctors, nurses and other healthcare staff all over the world. ...
What is reporting in nursing?
In medical circles, reporting refers to the act of transferring relevant information. In most cases, this information refers to the patient information that is transferred from one nurse to another during the change of shift. There are numerous occasions that require reporting.
Why is a mental health nursing report important?
It allows nurses and doctors to continue treating and providing care to their patients even when during shift interchange.
Why is it important to have an ICU nurse report?
Due to this, it is very important that nurses are able to gather the required information. To help with this situation, ICU Nursing Reports were brought into action. ICU Nursing Reports are used to obtain a list of essential details regarding the patient who has been admitted to the ICU.
What is the purpose of the General Information section in a nursing report?
This section is responsible for generating all the details regarding the patient such as Date of Birth, Gender etc. of the patient.
What is flow sheet in nursing?
A6. In simple terms, a flow sheet is a single or dual-page form, tasked with the job of gathering all important aspects of a patient’s condition. Similar to the other nursing reports, the flow sheet is tasked with gathering patient information.
What is a lab report?
Labs – Labs refers to the various patient reports which have been derived from the numerous tests conducted on the patient. The constituents of this section are Labs, Needed Labs, and Future Procedures. Completion – Completion is the final section of a nursing report template.
You Need a Nursing Brain Sheet That Works for YOU
For the longest time I have tried pushing the brain sheet that worked for me onto new students and newbie nurses. I’ve changed my tone.
The Nursing Brain Sheet Database
The response was AMAZING (to say the least). We received over 100 report sheet templates from nurses working in MedSurg, ICU, ED, OB, Peds, Tele . . . you name it.
1. Handoff and Nursing Report Sheet
This is the report sheet that my preceptor used to make me fill out prior to the end of each shift as a newbie. To be honest, at first I was so annoyed that I had to spend like an hour at the end of each shift filling this out. It wasn’t until I realized I was able to give a badass report that I was finally grateful she made me fill this out.
3. 4 Patient Simple Tele Sheet
Some people like it simple . . .this is the sheet for you. With slight prompting this sheet makes a great tool for the MedSurg or Tele nurse on the GO!
4. 4 Patient Simple Nurse Task Sheet
I love this one. At first glance it looks basic . . . put at closer inspection you start to see all the details and information you have available with it. From lab values, to foley care, to last pain med, this is would be a great one for a nurse that has a flow and just wants a simple push to stay a bit more organized.
5. Vertical Nurse Brain sheet with Assessment Diagram
I’m a visual learner. This one just grabs my attention. I like the top section for the “essentials” like blood sugars, DX, and Pt info. I also really like the area below the charts to draw little notes about your physical assessment. I really like this nursing brain sheet for beginner or experience nurse.
6. Just the Boxes
I’ll be honest . . . after a couple years of being a nurse my “brainsheet” has evolved into more of a few freehand drawing on a sheet of paper. If that sounds like you, this is probably the one for you. With little more than a few suggestions . . . this is a pretty basic organizer for nurses.
Popular Posts:
- 1. tulsa obgyn patient portal
- 2. nextgen patient portal tacoma
- 3. cecil family edicine patient portal
- 4. allegra arthritis associates patient portal
- 5. james bauer md patient "portal"
- 6. western missouri medical center patient portal
- 7. st thomas heart patient portal
- 8. promised land women's center patient portal login
- 9. huhs patient portal login
- 10. my patient portal boston children's